
John R. Perfect MD
Duke University Medical Center
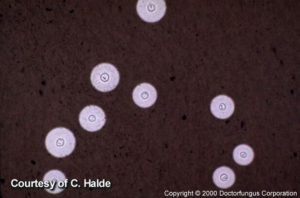
India Ink of CSF with C. neoformans

India Ink of CSF with C. neoformans
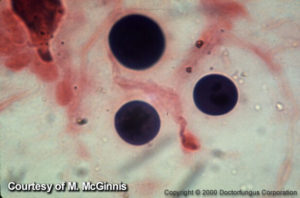
Gram Stain of tissue infected with C. neoformans
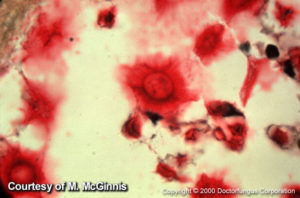
Mucicarmine stain of brain infected with C. neoformans
Introduction
From its first description in 1894-1895 as environmental yeast found in peach juice((A):125) to its identification as a clinical isolate causing osteomyelitis in a young lady ((A):22), this encapsulated yeast, Cryptococcus, has mirrored the study and growth of medical mycology worldwide. The major milestones of its history are chronicled in Table 1 and they span the entire last century. These events range from the clinical description of disease, identification of its life-cycle both environmentally and morphologically, its nomenclature (at least two pathogenic species), its development as a molecular model for fungal pathogenesis and its growth in diagnostic maneuvers and treatment strategies. In all these historical markers there are contained rich understandings regarding the disease which we characterize as cryptococcosis.
One of the critical features of cryptococcosis has been its meteoric rise in numbers of reported cases. In some respect, this rise might have been influenced by improved diagnosis and medical care but its massive increase in importance has more likely been a reflection of the dynamic change in the human host. As Littman and Zimmerman reported in the mid 1950’s there were less than 300 cases of cryptococcosis reported in the literature (78) but by the late 1970’s Kauffman and Blumer reported that cryptococcosis was the “awakening giant”(67). From their viewpoint at the Centers for Disease Control they could see the increased numbers of clinical isolates coming to their research laboratory. This realization marked the beginning of a three part major clinical outbreak of cryptococcosis (Table 2). This first outbreak started in the 1960-1980’s and was a reflection of the creation of modern medicine and its ability to immunocompromise hosts to treat life-threatening underlying diseases and to even produce immune tolerance to transplant organs. One of the collateral damages of these new found strategies to treat diseases was the growth of cryptococcosis. This outbreak of immune modulation continues today as we use immunosuppressants from steroids to monoclonal antibodies to abrogate the immune system which allows this yeast to reactivate its dormant infection and produce disease. The second big outbreak of cryptococcosis started in a simple manner in the 1980’s when there were reports of cases as opportunistic infections in patients with this newly recognized immunosuppressive syndrome called AIDS(143). With the expansion of the HIV infection epidemic and resulting AIDS, the reported cases of cryptococcosis grew substantially and the impact of these combined infections has recently reached an incredible number predicted by the Center for Disease Control of a million new cases of cryptococcosis per year with over 600,000 deaths per year worldwide (109) . This large epidemiological estimate makes it likely that cryptococcosis is the number one invasive mycosis today in regards to clinical disease and death worldwide (109). It is hoped that as HIV infection is controlled with HAART and its transmission reduction strategies, this number of cases will be reduced. In fact, in developed countries this assumption is already occurring (93) but cryptococcosis remains far from being controlled worldwide. The third major outbreak of cryptococcosis was first reported in the late 1990’s. A sudden expansion of cryptococcal cases in animals and humans occurred on Vancouver Island (69) and subsequently,this outbreak spread to mainland Vancouver, British Columbia and has finally reached into the Pacific Northwest, USA. This outbreak of cryptococcosis has been caused by a recombinant set of Cryptococcus gattii strains (47). These strains appear to have gained an increased virulence profile compared to their parental strain. Despite uncertainty regarding its expansion (robustness of yeast strains and/or increasing exposure, environmentally), there is a hypothesis that its ability to compete and flourish in a new environment was mediated by local climate changes (increased temperature and decreased moisture). This “perfect storm” of conditions has led to an outbreak of hundreds of cases in both immunosuppressed and apparently immunocompetent individuals (51) (85). Along with the other two cryptococcal outbreaks, this outbreak of disease continues without an apparent end to the ongoing events. Clearly, this invasive fungal infection is here to stay and produce disease for the immediate future.
In order to appreciate the massive growth in understandings of cryptococcosis three sentinel books on cryptococcosis measure and explain progression of disease: (1) Littman/Zimmerman, 1956 (78); (2) Casadevall/Perfect, 1998(25); (3) Heitman, Kwon-Chung, Kozel, Perfect, Casadevall, 2011 (58) and several other comprehensive reviews are also available (111) (95) (28) (Table 3). These books and reviews represent comprehensive, collated insights into the meanings of cryptococcosis for both the novice or the advanced student.
Organism
There are over 30 species that comprise this loosely aggregated genus first named by Kutzing in 1833 (Kutzing F. Algarum aguae dulcis germaniae decas III, New York Botanical Garden, 1833) and most are simply environmental yeasts with little impact on the human condition. In fact, even species like Cryptococcus laurentii and Cryptococcus albidus have rarely produced disease in humans (84) (59). Therefore, the primary focus of cryptococcosis resides in two species Cryptococcus neoformans and Cryptococcus gattii (73)Cryptococcus neoformans remains subdivided into two varieties Cryptococcus neoformans var. neoformans and Cryptococcus neoformans var. grubii (46). These two varieties have also been designated by their capsular serotype as D and A, respectively, with C. neoformans var. grubii (serotype A) producing the vast majority of disease worldwide. In fact, molecular studies suggest the two varieties are genetically separated from each other by approximately 20 million years(160).Cryptococcus gattii has also been designated by its capsular serotype as B and C. In recent studies on population genetics and clade analysis, Cryptococcus neoformans has been separated into 5 genotypes (VNI-IV, VNB) and similarly, Cryptococcus gattii has been divided into four genotypes (VGI-IV) and with further studies these genotypes are beginning to be further divided into specific subtypes (a-c). For example, the primary genotype for the Pacific Northwest outbreak is VGIIa with a recent identification of VGIIc strains in the Pacific Northwest USA. These genotypic division are helpful for ecological insights and will continue to be used to determine their evolutionary importance in the study of fungal pathogenesis. It is also important to note that C. neoformans and C. gattii are sibling species separated genetically from each other by greater than 40 million years (33). Therefore, these species have ecological differences such as bird guano-associated C. neoformans is not observed with C. gattii and although both are associated with trees and tree hollows in the environment, they are associated with different tree species such as the well-known eucalyptus trees as a C. gattii habitat (40). Furthermore, their sexual morphological structures (basidiospores) appear different; their biochemistry has definite differences; their genome sequence variations are up to 20% of their genome; and finally, their genetic networks or pathways can vary at certain sites for each species (103). There is no question that there has been some evolution occurring which begins to distinguish the differences in the biology of these two species. On the other hand, at present they are very similar in their human disease production(145),(94),(29). For instance, their basic virulence factors such as their capsule production, melanin synthesis, high temperature growth, urease production, phospholipase secretion are shared by both species. Despite several studies to compare and contrast the human disease produced by these two species, it is extremely hard to define precise differences and there is substantial overlap in both the clinical disease manifestations and treatment outcomes. Therefore, except for certain epidemiological factors, the ability to predict presentations or outcomes between the two species is clinically lacking and thus both strains are incorporated under the generic term cryptococcosis for clinical practice.
Cryptococcus is a heterothallic basidiomycete which can reproduce sexually (MAT “”alpha” and “a” strains) (72), unisexually,(61)with haploid fruiting or simply asexually, (159) (77)with yeast budding. The sexual forms are called Filobasidiella neoformans or Filobasidiella bacillosporus and both go through a mating cycle of yeast fusion, hyphal formation with clamp connections then formation of basidium with basidiospores . This sexual cycle generally occurs under relatively poor nutritional conditions when the yeasts are physically placed next to other yeasts. It is still not completely resolved whether these 1-2 micron-sized basidiospores or alternatively small, poorly encapsulated yeasts are the infectious propagules that are inhaled into the lung of the mammalian host. These spore structures are morphologically different and can initiate a different immune response than yeasts (153) (52). The basidiospores are an ideal size for alveolar deposition but once exposed to a nutritious food sources they rapidly convert into yeasts. Also, the sexual stage of cryptococcosis has not yet been morphologically identified in nature although observations of genetic recombination in nature support its presence (126).
The understandings around the pathogenesis of these yeasts from the organism viewpoint have exploded over the last decade. First, there are multiple well known virulence phenotypes to study such as capsule production, melanin synthesis, high temperature growth (37°C), urease production, phospholipase secretion, intracellular survival and proliferation, mitochondrial function and morphology (113). Second, with an efficient transformation system (150), genomes sequenced (82) and annotated, transcriptional (71)and proteomic profilings, population and individual genetic studies (80), a library of mutants (81) this encapsulated yeast has several hundred genes now identified through gene knock-outs and classic reverse genetics to be essential for its virulence composite(113) . These genetic studies have spanned a variety of topics from sexual morphogenesis; control of specific phenotypic signaling pathways; gene regulations; basic understandings of cell metabolism for stress growth and survival; and apoptosis/autophagy (58). One new area of understanding is beginning to emerge and that is the area of micro-evolution and how the host environment with its stresses promote these genetic changes. For years, we have known about phenotypic switching in C. neoformans (49) but the flexibility or plasticity of the cryptococcal genome in vivo may have major relevance to this organism’s adaptation at the site of infection and even lead to in vivo aneuploidy states which as a consequence can lead to antifungal drug heteroresistance, alterations in virulence fitness and either appearance of multiple strains or variants infecting the host (33;34;49;140). The dynamic genetic mechanisms for rapid change of this yeast without plasmids but with transposible elements and epigenetic factors may be the new frontier of understanding why it is an efficient pathogen. Clearly, the molecular understandings are beginning to strip away the cloak of secrecy about what makes this sugar-coated yeast such a deadly pathogen. Third, this yeast has a wide host range for infection and production of disease. Therefore, there are very robust(animal) host models for study of cryptococcal disease and these include worms (C. elegans) (99) ameba (147) wax moth grub (Galleria), zebrafish, guinea pigs, rats, mice, and rabbits (26). In many respects, these animal models ideally support the molecular manipulations of this yeast to further gain understanding of this fungal disease. The results of this work will likely yield pathobiological insights for identification of new antifungal drug target(s) for treatment and/or vaccine(s) for preventive and therapeutic management strategies. Although this yeast is not a known pathogen for plants, it can grow, mate and survive well on leaves which may be one its major ecological niches (161). Furthermore, it does appear to have developed features for it to colonize predatory invertebrates in nature (ameba and worms) (147) and these survival skills may have been adapted for use in the mammalian host. Finally, it is also a well-known mammalian pathogen with veterinarian consequences from local disease such as cow mastitis (118) to nasal infection in dogs/cats (86) to widely disseminated disease with central nervous system localization in animals as is observed so frequently in humans with invasive disease (26).
Host
The importance of host immunity to the development of cryptococcosis is the single most critical feature of this infection from diagnosis to prognosis (28), (58), (112). A major pathological principle in understanding of cryptococcosis is that many individuals are infected with this yeast but their immune system controls the infection with minor and insignificant symptoms. However, like tuberculosis, the yeast can persist in tissue (dormancy) for long periods of time to then reactivate and produce disease during an immunosuppressive event. A half-century old autopsy study has supported this asymptomatic pulmonary lymph node-complex scenario (9). Furthermore, this reactivation scenario has been supported by recent observations with HIV infection progression to low CD4 counts (50-100 CD4 cells/ul) and this immunosuppressive lymphopenia directly linked with higher risk of cryptococcosis as the reduction of cell-mediated immune cells occurs (31). Furthermore, iatrogenic immunosuppression with high dose corticosteroids and recently, immunosuppressive monoclonal antibody treatments (etanercept, infliximab, alemtuzumab) (151) are definitely linked to cryptococcal disease . Therefore, the host immune status remains a critical factor for the clinician in diagnosis and prognosis.
There are a series of well-known risk factors associated with cryptococcal disease. In Table 2 there is a listing of predisposing factors for cryptococcosis. Clearly, the two highest risk factors are HIV infection and corticosteroid use. The corticosteroid use as a risk factor incorporates most of the transplant recipients and particularly, the solid organ transplants with their long term corticosteroid exposure and relatively high daily doses (> 20mg/day of prednisone) (62), (128), (137), (155). Among the other risk factors that require some discussion are the lymphomas/chronic leukemias and the connective tissue diseases in which most of these cases are aided by corticosteroid usage. The monoclonal antibodies have become the “new risk factor” for mycoses like cryptococcosis and histoplasmosis (151). Diabetes continues to be present in a large number of patients with cryptococcosis (108) but explanations for its underlying presence or how to clinically use it as a risk factor are less precise. On the other hand, cirrhotic patients or those with cryptococcosis in the presence of severe liver disease may have the worst prognosis either through delay in diagnosis or the end stage of liver disease at diagnosis (135). Pregnancy is not a severe immunosuppressive event but its immunological perturbations can manifest with the occurrence of cryptococcal disease but also the appearance of IRIS in the post-partum setting (117), (6), (41), (138). On the other hand, although cryptococcosis can occur in children and specifically, those with certain risk factors, present reports suggest that it is probably much less common then in adults(1), (54), (89), (76) (141),(27) ,(55). The host status through identification of specific underlying diseases or risk factors is a major instrument for help to the clinician in the diagnosis of cryptococcosis since it is used to amplify the aggressiveness for identification of this infection.
It should be noted, however, that not all patients with cryptococcosis have an underlying disease. In fact, if you exclude HIV- infected patients, approximately 20-30% of patients with disseminated cryptococcosis will present with no apparent underlying diseases or known risk factors (108). Since the host is classically protected by a vigorous Th1 response, it is likely that those with no apparent underlying disease but who develop disseminated cryptococcosis do, in fact, have some undetected alterations in their protective immune responses. A small genetic susceptibility study through identification of DNA polymorphisms in certain immune genes has been started (91) but clearly, further comprehensive studies in genetic susceptibility and immune functions will be necessary for us to get a true appreciation for what is really going on in the apparently normal host with disseminated cryptococcosis. In fact, at times, the dysregulated immune systems and heterogenerous populations of patients makes this group of patients (apparently normal hosts)the hardest to manage since they may have late disease (prolonged disease because of delayed diagnosis) with either a high burden of organisms before treatment and/or prone to the development of a very aggressive immune reconstitution inflammatory syndrome ( IRIS). In this group of apparently normal hosts with cryptococcosis, it is reasonable to check for underlying HIV infection since it is a treatable illness and also it is probably reasonable to obtain a total CD4 lymphocyte count to identify patients with idiopathic CD4 lymphocytopenia which may require prolonged antifungal suppressive therapy, although present data suggest that this idiopathic syndrome with cryptococcosis actually has a good prognosis(162).
The general theme of immunity for this disease is that prevention of disseminated cryptococcosis is controlled by an efficient cell-mediated immunity. This fact is supported by many in vitro studies, animal models and all present cytokine studies in humans (132). For instance, defective production of interferon gamma and TNF-alpha but not IL-10 occurs in patients who have cryptococcosis which indicates a shifting to a predominant Th2 host response(21),(39) . Furthermore, during effective treatment at the CNS site of a cryptococcal infection, an up-regulated Th1 response occurs as measured by higher CSF interferon gamma levels and lower CSF yeast counts (133). In fact, this cytokine elevation at the site of infection
(16) or the (exogenous) systemic administration of recombinant gamma interferon can correlate with an improved clinical response (107).
Much of the host issues for diagnosis and initial management of cryptococcosis are based around a deficiency in host responses and the risk groups identify this focus. However, it is essential that clinicians realize that the total management of cryptococcosis must deal with the total immune dysregulation that occurs and not just its early deficiencies. This is emphasized by the many pleomorphic effects of the lingering cryptococcal polysaccharide can have on host immune functions (116). Thus, even the yeast and its products can modulate the host environment. This immune dysregulation was clearly identified during the AIDS epidemic with cryptococcosis and the use of HAART for HIV infection during cryptococcosis(130). The dramatic identification of immune reconstitution inflammatory syndrome (IRIS) was clearly described. IRIS can occur in 2 forms: (1) “unmasking” IRIS in which undiagnosed cryptococcal symptoms appear after the start of HAART; or (2) “paradoxical” IRIS during the treatment of known cryptococcosis and administration of HAART (130). Clinicians deal with disease and at times a too aggressive inflammatory response (particularly in CNS) can cause further disease such as elevated intracranial pressure. IRIS is not limited to HIV-infected patients regaining their immune cells with HAART but is described as a complication in solid organ transplants receiving potent immunosuppressive regimens which might be altered during management of infection (136)and can also occur in apparently normal hosts as they are started on treatment for cryptococcosis (38). These cases of IRIS and cryptococcosis classically emphasize the principle of the “Goldilock’s “ paradigm of immunity: immune responses can be too little or too much and contribute to disease; an immune response needs to get it just right to be successful.” Fungal diseases like cryptococcosis occur within this immunological paradigm (37).
IRIS in cryptococcosis has been well-described in multiple reviews with symptoms, timing of appearance, and general incidence of disease (139). That said, it is still a clinical judgment at the bedside about its diagnosis and management. Unfortunately, there are not yet an immunological testing system to assure clinicians of how the host immune system is performing on a real time basis and general markers of inflammation may suggest it (19) but they are not precise in their diagnostic or therapeutic worth for IRIS at present (139). Thus treatment of IRIS becomes an empirical art form of medicine rather than directed by evidence-based guidelines. However, the concept of a complicating IRIS occurrence cannot be ignored in management strategies of cryptococcosis.
Laboratory Diagnosis
Once cryptococcosis is considered in the differential diagnosis of an infectious disease there are very good tools to diagnose it. Histopathology can be relatively distinctive with the capsule around the yeasts identified by alcian blue or mucicarmine stains and a Fontana-Masson stain can identify melanin production. These 5-20um budding or single yeasts can clearly be seen in the low-cost colloidal medium of an initial India ink examination on cerebrospinal fluid that can be positive in up to 80% of HIV-infected patients with cryptococcal meningoencephalitis and with careful examination can be positive in 50% of non-HIV infected patients. This is generally related to burden of yeasts and frequently patients with AIDS and disseminated cryptococcosis will have a large burden of yeasts in CSF that can range between 106-107CFU of yeasts/ml. The India ink examination has difficulty in identifying yeasts when their concentrations drop to 103 CFU of yeasts/ml or lower. There are some clinical cases and this is more commonly reported in the lung where the histopathology has some difficulty in detecting small capsules (57) (121). However, it is still likely that a capsule is present since an acapsular mutant is uniformly avirulent.There are a series of non -specific stains which might identify this yeast and particularly calcofluor and Gomori’s methenamine silver stains which represent classic fungal stains will identify this yeast in tissue. There are culture, molecular, and antibody methods to distinguish C. neoformans from C. gattii but at present except for epidemiological purposes it is not clear that separating an isolate into specific species is a necessary requirement of the laboratory to help clinical management of the patient.
The serologies of cryptococcosis for diagnosis have been very well studied. Serum cryptococcal antibodies are not particularly helpful in diagnosing and deciding treatment for cryptococcosis and therefore are not used clinically. These antibodies, however, are useful for epidemiological studies of exposure and their presence may actually suggest a good prognostic sign (53). On the other hand, the detection of cryptococcal capsular polysaccharide antigen in serum or CSF has performed extraordinarily well in diagnosis for many years (114) (26). It is one of the premier diagnostic tests in all of medical mycology. There is also some correlation between antigen load and burden of viable yeasts in the host prior to treatment so the height of the antigen titer may have some prognostic features (123). There are primarily two types of commercial tests, latex agglutination and ELISA systems. The sensitivity and specificity of these tests are above 90% and although there are occasional false positives or false negatives, these results can frequently be sorted out with careful repeat testing or confirmatory culture results. Therefore, in areas where this fungus is endemic, any subacute or chronic meningitis case should have a CSF cryptococcal polysaccharide antigen test performed. It is rapid and accurate. Despite its diagnostic utility and possessing some general prognostic features on initial titer, the cryptococcal antigen test is not very precise for use in following therapy (63). It is a large molecule with many immunological effects but the exact kinetics of its elimination from the body are variable and not precisely predictive of success. All clinicians would like to see the antigen eliminated from the host with successful therapy but treatment decisions cannot be directly linked to the quantitative antigen measurement. The term isolated cryptococcal polysaccharidemia describes a condition in very high-risk patients primarily those with HIV infection who have a positive cryptococcal antigen titer and no positive cultures or prominent symptoms (63), (87). In these patients the incidence of eventually developing cryptococcosis is very high and in most patients an examination of CSF is warranted and even if negative, administration of empiric antifungal therapy should be considered.
The use of the cryptococcal antigen in a high prevalence area such as sub-Saharan Africa as a screening device has great appeal if it could be cheap and easily performed. There is now a Lateral Flow Test being studied and marketed which has the great potential to be cheap and could use finger stick blood or urine. It is very low tech as a simple dipstick test and has an easy storage requirement. There are now prospective data that in those HIV-infected patients that have a negative cryptococcal antigen test are unlikely to develop cryptococcosis over the next year (63). A positive cryptococcal antigen test will need a lumbar puncture work up to rule out CNS disease and even with negative CNS disease but a positive test, it probably supports antifungal treatment until HAART returns improved host immunity. This simple Lateral Flow Test could have a profound effect on new management strategies for the vast number of patients with this disease. It simply needs to be integrated into the health care systems in resource-limited environments. All these issues are being examined at present.
Finally, the yeast is relatively easy to culture on standard media with growth in 2-10 days and it can be isolated from blood culture systems. Although quantitative CSF yeast counts have excellent predictive value for therapeutic outcome in research studies (16) (20) they have yet to be incorporated into clinical practice. In fact, future strategies should consider measurement of the rate of yeast decline in CSF as a judge to success of induction therapy (14) and its length.
Clinical Manifestations
This yeast can produce disease in every organ of the human body and widely disseminated cryptococcal infection can occur in multiple organs in patients who are severely immunosuppressed. There have been several studies which have examined the differences in clinical manifestations between C. neoformans and C. gattii and the general summary is that both species can produce similar symptoms and most of the symptoms are simply controlled by the host’s immunity (145) (94) (29). However, it is interesting to mention that C. gattii can frequently cause disease in primarily immunocompetent hosts who have prominent inflammatory masses and these produce cryptococcomas that may require surgery or prolonged antifungal therapy in their management strategies.
The clinical differences between those with or without an underlying HIV infection display the degree of host immunodeficiency and there are general trends. HIV-associated cryptococcosis produces more CNS and extra pulmonary involvement, higher rates of positive India ink examinations, more positive blood cultures and fewer CSF inflammatory cells. Clearly, patients with HIV infection commonly present with a high burden of yeasts and poor inflammatory responses. The speed and magnitude of symptoms can have a wide-range but there are general trends. For instance, symptoms are generally subacute (weeks) to chronic (months) and although severity can be extreme with septicemia symptoms or coma, the majority of patients present with persistent subacute to chronic headaches or chronic pulmonary complaints. The timing of symptoms are frequently linked to severity of immune depression. With more rapid symptoms in the more severely immunosuppressed hosts. There are multiple reviews which detail the clinical issues around cryptococcosis but the following sections describe specific issues around the major sites of disease, pulmonary and central nervous systems, and other less common body sites (28).
Pulmonary
Pulmonary cryptococcosis varies in its presentation from an asymptomatic infection as a simple yeast colonization of the airway or an abnormal radiograph as a solitary nodule which mimics lung cancer to a life-threatening fungal pneumonia presenting as an acute respiratory distress syndrome (156), (157). Acute pulmonary cryptococcosis can manifest with an abnormal chest radiograph and very minimal symptoms or in fact, is asymptomatic but can also present with symptoms of pneumonia (fever, cough, and sputum production) (92), (68), (100), (8). Radiographic presentations are varied. They include single or multiple pulmonary nodules (most frequent), with or without cavitations, parenchymal consolidations and interstitial infiltrates. Other radiographic findings include pleural effusions, hilar lymphadenopathy, diffuse reticulonodular opacities, endobronchial lesions resulting in airway obstruction with lung collapse and findings which mimic either primary or metastatic cancers. In severely immunosuppressed patients there may be overlap with other infections such as pneumocytosis and in fact, commonly in these severely immunosuppressed patients, they will present with CNS rather than pulmonary symptoms. Although not a precise marker, a cryptococcal polysaccharide antigen is usually negative when infection is confined to the lung and a positive serum cryptococcal antigen test makes dissemination of infection from the lung more likely. Although early CNS cryptococcosis can be relatively asymptomatic and yet a propensity for CNS involvement is unique and important to management, years of clinical experience have now allowed us to recommend that asymptomatic patients who are immunocompetent and with a negative serum polysaccharide antigen who are found to have cryptococcal lung involvement do not necessarily need a screening lumbar puncture to rule out CNS disease (2),(8) . However in immunosuppressed patients, those with pulmonary cryptococcosis should probably have a lumbar puncture to rule out CNS disease regardless of symptoms since identification of CNS involvement would involve different treatment strategies (134).
Central Nervous System
Both C. neoformans and C. gattii have a propensity to invade the central nervous system. The reasons for this clinical observation remain an area of active investigation but the consequences are clearly delineated in that meningoencephalitis is life-threatening with 100% mortality if untreated, (98) 40-70% mortality in less-resourced medical settings with inferior treatments (127) (65) and in advanced medical settings and despite excellent treatment guidelines, a mortality rate of approximately 20% (152). Symptoms and signs may occur for several weeks to months and include headaches, fevers, and cranial neuropathies, alteration of consciousness, lethargy, memory loss, meningeal irritation signs and finally coma. At times, these symptoms may present in several days with patients known to be severely immunosuppressed like HIV-infected individuals. One of the real difficult diagnostic challenges for cryptococcal meningoencephalitis occurs in an apparently normal host with a subacute dementia. Without specific risk factors, the non-descript presentation can delay diagnosis and potentially lead to a poor prognosis despite the lack of a serious underlying disease. While patients who appear to be immunocompetent presented with meningitis as their marker for disseminated disease with a lower rate of fungemia and mortality, they still do frequently come to a diagnosis with a longer mean time of illness and with a concomitant more intense inflammatory responses . Thus, at times, these patients can be very difficult to manage with substantial morbidity (38).
There are several important clinical issues in meningoencephalitis management. First, measurement of intracranial pressure is essential (56). Increased intracranial pressure may occur at three time periods with cryptococcal meningoencephalitis: (1) at initial diagnosis with a large burden of yeasts and/or profound host inflammatory reaction; (2) during initial induction antifungal therapy in which clumping and dying yeasts with large amounts of polysaccharide in CSF and tissue combine to obstruct CSF outflow or with the introduction of HAART or reduction in iatrogenic immunosuppressives allows an exaggerated immune reaction that leads to cerebral edema; (3) finally, after the initial infection appears controlled, there is development of signs of classic obstructive hydrocephalus that is caused by residual scarring with resolution of infection. Unfortunately, management guidelines for increased intracranial pressure remain empirical and not precise but attention to increased intracranial pressure can determine success (112).
Second, the recognition of the appearance of IRIS is important. It is a consequence of the dramatic swings in the immunologic responses in these patients. The most dramatic occurrence of this syndrome occurs in HIV-infected patients as they improve their immunity with HAART. However, attention to this well-described complication of cryptococcal meningoencephalitis in HIV-infected individuals should not obscure the fact that IRIS is a frequent and difficult management issue in transplant recipients when their immune suppression is dialed down or even in apparently normal hosts as yeasts are killed and antigen is being eliminated from tissue (136). Unfortunately, with IRIS it has no precise laboratory markers of its existence and therefore must be diagnosed at the bedside with clinical features. The general definition of IRIS is a condition when new or worsening clinical or radiographic manifestations occur that are consistent with an inflammatory process but there are negative or declining fungal biomarkers or cultures. This can occur in up to 30-35% of HIV-infected patients who have HAART initiated with decreasing viral loads and rising CD4 counts and the timing of occurrence can be wide (64), (88), (142), (83). In non-HIV, it is even less precise in its natural history but occurs in approximately 5% of patients with cryptococcal meningoencephalitis who have a solid organ transplant. In this population the timing of IRIS ranges from 4-12 weeks after starting therapy and it may be related to the reduction of the patient’s anti-rejection medications (136). Clearly, this is the dilemma of the clinician to reduce immunosuppression to help the host eradicate the fungal infection but on the other hand, be able to identify and control an over-committed immune response which might further produce disease in the host. In the CNS, IRIS can have profound consequences with significant morbidity and mortality if not appreciated and managed. IRIS represents the two-edged sword of management since successful outcomes require effective immunity to eliminate cryptococcus but not too much which can also cause disease.
Third, brain parenchymal lesions (cryptococcomas) may complicate meningoencephalitis. C.gattii tends to have a higher predilection to cause cryptococcomas than C. neoformans in these brain masses with high intracranial pressure, cranial neuropathies, hydrocephalus, and a slower response to antifungal therapy. These cryptococcomas can be solitary or multiple and their sizes may vary from less than to more than 3cm. Importantly, radiographic detection of these successfully managed masses may persist for long periods of time despite adequate treatment (60) and in fact, persistence of cryptococcomas on radiographs may last for over a year. In severely immunosuppressed patients there are rare reports of individuals who have cryptococcal meningitis but a concomitant brain abscess caused by other pathogens such as Nocardia. Therefore, large brain masses (>3cm) may require surgical exploration to help treat brain lesions but at times to also make the diagnosis of another infectious disease agent.
Other Body Sites
There are several other body sites of cryptococcal disease that require some specific attention . First, skin cryptococcosis can occasionally be caused by direct inoculation and thus represents primary disease. Primary cutaneous cryptococcosis presents as a whitlow or
phlegmon with a history of skin injury, exposure to bird droppings and isolation of acneiform from the lesion (102). However, in most cases the development of cryptococcal skin disease reflects a site of disseminated infection. In general, cutaneous cryptococcosis can present with almost any type of skin lesion. These lesions include acneform lesion, purpura, vesicles, nodules, abscesses, ulcers, granulomas, pustules, draining sinuses and cellulitis (79). Therefore, clinically by visual inspection, it will not be possible to determine cryptococcal involvement without a proper skin biopsy for culture and histopathology. Even a characteristic skin lesion for cutaneous cryptococcosis in HIV-infected patients of a papule or maculopapule with central ulceration that has been described as a “moluscum contagiosum-like lesion” can also be produced by Histoplasma capsulatum, Coccidioides immitis/posadaii or Penicillium marneffei. There are interesting cases of cutaneous cryptococcosis with strain features of lower temperature growth and skin tropisms (144) and certain epidemiological features in which appearance of lesions in the skin was associated with the use of calcineurin inhibitors and their known ability to affect high temperature growth in this yeast(104).
Second, prostatic cryptococcosis is generally asymptomatic and has been considered a site for occult or sequestered infection that is protected from antifungal treatments(74). Latent prostatic cryptococcosis has been uncovered in the blood after prostatic surgery (13) and even serum prostatic-specific antigen has been elevated with chronic infection of the prostate with cryptococcus. The most dramatic cases of prostatic cryptococcosis were reported as relapsed sites early in the AIDS epidemic and prior to widespread use of HAART. Thus, this organ may be an important site for relapsed infection if therapy is discontinued early or immune reconstitution has not occurred.
Third, ocular cryptococcosis has been reported in up to 45% of patients with cryptococcosis and thus becomes a significant site for disease (104). The most common manifestations are ocular palsies, papilledema and blindness but in severely immunosuppressed patients retinal lesions with or without vitritis may appear. Furthermore, catastrophic loss of vision without evidence of endophthalmitis also occurs(17), (120). Visual loss which is a serious sequelae of cryptococcal meningoencephalitis can be caused by three pathogenic processes. The first process is caused by infiltration of the optic nerve and produces a rapid visual loss with few effective treatments. The second process is invasion of the retinal area and extension into the vitreous body and this also has high a rate of permanent visual loss but may be more responsive to antifungal therapy. The third process is caused by increased intracranial pressure and leads to a slower visual loss and this loss may be prevented or slowed down through placement of ventricular shunts.
Most other body sites have descriptions that are so few and limited that they provide few insights into disease. For instance, cryptococcus has caused myositis, genital-lesions, hepatitis, thyroiditis, adrenal mass, gingivitis, sinusitis, salivary gland involvement, neck masses, esophagitis, biliary tract involvement, enteritis, mastitis, breast masses, lymphadenopathy. However, there are several areas which deserve some special mention. Cryptococcal infection of the bone and joints can present with osteolytic lesions or evidence of acute/chronic arthritis, respectively, and there has been some association for these infections with sarcoidosis (10). Cryptococcal peritonitis has been well- described (45) (4). It may present in the ascites of chronic liver disease or in the peritoneal dialysate of patients with chronic renal disease (35). Interestingly, cryptococcuria occurs and even pyelonephritis is described but the urinary tract site is less common than one would expect with severely disseminated disease and may simply reflect the length of routine culture methods. Cryptococcemia in the severely immunosuppressed patients, like those with advanced HIV infection, is relatively common and generally reflects a large burden of yeast in the host. Despite frequent cryptococcemia, the reported cases of cryptococcal endocarditis are less than a dozen and this includes both native and prosthetic value endocarditis. Although not a particularly “sticky“organism with its capsule, it can produce biofilms but rarely is reported to infect prosthesis (foreign bodies).
Management
The bipolar existence of cryptococcal guidelines runs the spectrum from the best-evidenced fungal disease to major gaps in our knowledge base. In 2000, the Infectious Disease Society IDSA of America proposed the Practice Guidelines for the Management of Cryptococcal Disease which compiled some general agreements about recommendations for treatment (122). In fact, one report suggested that following these guidelines produced a positive outcome (131). A decade later in 2010 the revised IDSA Guidelines were published in response to a little more data and the ability to organize the patient groups and special issues in a more direct manner (112). From this framework of clinical questions, there were 86 recommendations made to help merge recent and established evidence-based data along with shared expert clinical opinions and insights. The following represents a synopsis of these Guidelines and for an in depth discussion of the guidelines the reader is referred to the document (112).
The 2010 Cryptococcal Guidelines are arranged in the following manner. The issues around cryptococcal meningoencephalitis are best separated out into three patient groups and these are HIV-infected patients, transplant recipients, and those that are non-HIV and non-transplant. With this substrate the detailed recommendations for cryptococcal meningoencephalitis management of each group are displayed in tables 5-7 and table 8 includes recommendations for the management of non-meningeal cryptococcosis which primarily focuses on pulmonary disease but there are other issues approached for the non-meningeal, non-pulmonary cryptococcal diseases including fungemia. Importantly, in these guidelines there are discussions regarding special clinical situations (pregnant women, children, persons in a resource-limited environments and C. gattii-infected individuals). There was also an attempt to approach management of infectious complications and in this area there were guidelines provided for: (1) persistence and relapse of disease; (2) elevated intracranial pressure; (3) IRIS; (4) mass lesions (cryptococcomas). In this document all these areas were examined and careful insights were provided.
Within the 86 recommendations there were specific limitations. First, the management of increased acute intracranial pressure is emphasized in its importance (106), (56), (149) but specific guidelines created on evidence-based studies is sorely lacking and therefore, general suggestions about repeated lumbar puncture are made but are not precise . Second, recent data with present antifungal regimens in the management of non-HIV and non-transplant cryptococcal meningoencephalitis are based on a combination of old studies and extrapolation from studies in HIV-infected patients because new studies on this risk group are meager. Third, at this point there is no comparative data to determine whether disease by C.gattii should be treated the same or different from C. neoformans and by default present guidelines suggest they should be treated similarly. Fourth, the timing of administration of HARRT during treatment of cryptococcal meningoencephalitis needs better definitions and the guidelines give a range from 2-10 weeks until evidence-based studies better define their use. Fifth, immune modulation with recombinant gamma interferon has been studied in primary induction therapy (107)but in the guidelines it is recommended for salvage or resistant disease so its use and impact still remain uncertain. Sixth, IRIS is probably more common than is reported and its diagnosis is imprecise, but once considered, when to treat with anti-inflammatories like corticosteroids is simply left to the clinician. Once the decision to treat IRIS is made, the dose and duration of steroids is empirical. Seventh, it is likely that present guidelines will remain in a similar place for the most part over the next decade because there are no new drugs or few new robust strategies in study. Despite some of these concerns about the guidelines they do provide a “flag in the sand” document for all clinicians to base their practice. In fact, when there has been a retrospective review of guideline use, there does appear to be an improved outcome (131). However, they should still be challenged and improved upon with evidence-based studies. We still have in high-resourced medical systems an 18-25% mortality for disseminated cryptococcosis and that remains too high.
These guidelines and the general philosophy of cryptococcal management is based around three important principles: (1) Initial aggressive induction therapy to rapidly and efficiently reduce the burden of yeasts (15); (2)Recognize and manage IRIS (Immunity is deficient and can also be over abundant and we must try to get it just right); (3) Adequate control of the underlying disease when present. Therefore, the management of cryptococcosis remains a combination of both “clinical science” “ fact and bedside medical” art with an influence from local practices and resources.
Prognosis in cryptococcal meningoencephalities has some features which the clinician needs to consider as treatment is begun. It is primarily based on the underlying diseases (liver disease vs. cancer vs. HIV infection), burden of organisms (high number of viable yeasts such as >106 CFU/ml of CSF or high cryptococal antigen titer ? 1:1024), symptoms at presentation (coma) and the host inflammatory reactions (CSF leukopenia). Specific factors for a poor prognosis include: (1) comatose state; (2) high antigen titer and/or heavily positive India ink; (3) low number of CSF inflammatory cell (< 20cells/ul) ; (4) symptomatic elevated intracranial pressure; (5) underlying diseases such as poor prognosis with liver diseases to those with solid organ transplants that have variable outcomes.
The future for new fungicidal regimens in the treatment of cryptococcosis remain meager but the ability to study new agents and strategies has never been more efficient and insightful with a limited number of patients using serial quantitative yeast counts in the CSF. This technique has now been validated in several studies (16) (20). Clearly, without effective treatment the natural history of cryptococcal meningoencephalitis in immunosuppressed individuals in poor-resourced environments is a rapid downhill spiral to death after coming to medical attention (98).
Prevention
There are several methods for preventing cryptococcosis. First, patients with HIV infection can dramatically reduce their incidence of cryptococcal disease by the use of appropriate HAART. Second, HIV-infected individuals with low CD4 counts (<100 cells/ul) can reduce their incidence of cryptococcosis with fluconazole prophylaxis (119) (90). Third, a very high-risk patient might avoid high risk environmental exposures such as bird droppings or certain trees in endemic areas. Finally, there have been studies of cryptococcal vaccines such as a GXM-protein conjugate which protects animals (18). However, future emphasis in this area will need to approach efficacy, risk- patient assessment and cost-benefit analysis.
Table1: Landmarks in the Clinical History of Cryptococcosis
| Date | Happening | Importance | Reference |
|---|---|---|---|
| 1895 | First clinical case description of C.neoformans | Cryptococcus causes human disease, disseminates in body, and fatal infection | ((A):22;24),(23) |
| 1896 | Clinical disease caused by C. gattii | Disease caused by more than one strain | (32) |
| 1902 | Horse infection | Host range of infection includes mammals beside humans | (50) |
| 1906-1916 | Description of CNS cryptococcosis | The beginning of the clinical features of cryptococcus in the central nervous system | (154) |
| 1935 | First mycological classification of cryptococcosis | The creation of mycological and taxonomic structure of genus along with appreciation that there were four serotypes | (11) |
| 1951-1955 | Isolation of cryptococcus from soil and bird guano | The ability to find yeast in the environmental traffic of humans | (42;158) |
| 1952 | Prolonged ,untreated cryptococcosis of CNS | Appreciation that this yeast can persist in body for a prolonged period of time | (44) |
| 1955 | First case of cryptococcal meningitis successfully treated with Amphotricin B (AmB) | The beginning of the era for successful treatment of invasive mycoses and specifically, fatal CNS cryptococcosis | (7) |
| 1955 | Autopsy studies show lung/lymph node complex | Supports the dormancy theory of cryptococcosis | (9) |
| 1960-1965 | Relationship of pigeons to Cryptococcus neoformans clarified | Littman carries out several seminal studies establishing that pigeon guano is a fertile site for the growth of C. neoformans in cities. | ((A):78) |
| 1962 | Development of bird seed agar | Staib develops a new agar type that facilitates identification of C. neoformans in clinical end environmental samples | (146) |
| 1968 | Creation of cryptococcal polysaccharide antigen test | One of the best diagnostic and prognostic fungal test available to clinicians today | (66;101) |
| 1975 | Identification of the perfect state | Major understanding of life-cycle with implication for genetics, evolution and transmission | (72) |
| 1978 | Recovery of H99 from a patient in North Carolina | This strain becomes the prototypical C. neoformans var. grubii strain and by the early 21st century is widely used in experimental studies | (111;115) |
| 1979 | Randomized, prospective trial comparing AmB vs AmB + 5FC for cryptococcal meningoencephalitis | A new standard for antifungal therapy; successful introduction of combination therapy for invasive mycoses | (12) |
| 1983-4 | Link established between AIDS and cryptococcosis although AIDS first clinically described in 1981 by 1984 clearly AIDS opportunistic infections included cryptococcosis | HIV infection remains the single biggest risk factor for appearance of cryptococcal disease in the world today | ((A):143) |
| 1987 | Generation of the first monoclonal antibodies to C. neoformans capsular polysaccharide | The availability of mAbs to C. neoformans allowed new approaches to the study of capsular antigenic structure and to analyze the contribution of humoral immunity to host defense. The pioneering work of Dromer describing the first protective mAb catalyzes numerous studies in the 1990s | (96) |
| 1990 | Cryptococcus found to be associated eucalyptus trees | The identification of trees as an environmental source for this fungus | (40) |
| 1990-1999 | Monoclonal anticapsular antibody can have positive impact on disease | Beginning in 1991 several laboratories employ mAbs to dissect the role of humoral immunity in host defense. This work establishes a new paradigm whereby antibody-mediated immunity can be useful against intracellular pathogens. | (96) |
| 1990-1999 | Cell-mediated immunity established to have critical role in host defense | Although granuloma formation had long been established as the effective tissue reaction, several laboratories conclusively associated cell mediated immunity with host defense in the 1990s. | (75;97) |
| 1990-1999 | Mechanisms of polysaccharide-mediated immunosuppression identified | Numerous laboratories show that capsular polysaccharide has protean immunomodulatory effects | (25) |
| 1992-3 | Development of a transformation system | Opened molecular studies on cryptococcal virulence composite | (150) |
| 1993 | A capsular-conjugated vaccine was protective in mice | Principle of protective fungal vaccine is theoretically possible | (35) |
| 1994-1997 | Creation of capsule, melanin, and high temperature growth mutants | Use of site-directed mutants to study the major virulence phenotypes | (104;124) |
| 1994 | Standard polysaccharide structural motifs assigned | After more than two decades of investigation by several laboratories Cherniak and Sunstrum propose that six mannose triads are responsible for polysaccharide structure. | (30) |
| 1997 | Integration of induction, consolidation and suppressive phases of treatment for meningoencephalitis | Allowed a strategy for initial aggressive fungicidal approach with prolonged therapy for residual disease | (152) |
| 1998 | Indentification of haploid fruiting | Morphologic/life-cycle features with epidemiologic implications | (77;159) |
| 1998 | Description of phenotypic switching in C. neoformans | The ability of C. neoformans for morphological change is associated with changes in virulence and persistence | (48) |
| 2000 | C. neoformans established as a facultative intracellular pathogen | Although C. neoformans was known to replicate inside phagocytes in vitro since the 1960s the recognition that this occurred in vivo ushered in a new phase of pathogenesis studies. | (43) |
| 2001 | Virulence hypothesized to emerge from protista interactions | Provided an explanation for the ready-made virulence of C. neoformans in soils and led to the exploration of several alternative non-mammalian host systems | |
| 2002 | Outbreak of C. gattii infection in humans and animals identified | An ecological/environmental shift in habitat and infects apparently normal hosts. | (69) |
| 2004 | Gamma interferon used as adjunctive therapy in meningitis | First randomized trial with the use of immune modulators for fungal treatment | (107) |
| 2005 | Genome of C. neoformans sequenced | C. neoformans studies can go genome wide | (82) |
| 2005 | Classification of two pathogenic species | C. neoformans and C. gattii considered evolved into separate species for taxonomy purposes | (73) |
| 2005 | Clinical description of IRIS with HAART | IRIS is a major clinical condition in AIDS, organ transplant recipients and normal hosts | (83;129) |
| 2005 | C. gattii outbreak strains found to represent recombinants with improved fitness | Example of same sex mating and creation in nature producing hyper- virulent strains and clinical outbreak | (47) |
| 2006 | Non-lytic exocytosis of C. neoformans from phagocytic cells | C. neoformans provides a new paradigm in host-microbe interactions by demonstrating non-lytic exit from infected cells. | (5) |
| 2010 | Infectious Disease Society of American (IDSA) Cryptococcal Treatment guidelines | Updated comprehensive version of the previous 2000 IDSA guidelines | (110) |
Table 2: Outbreaks of Cryptococcal Disease
| Description | Epidemiology | Pathogenesis | Outcome | Ref |
|---|---|---|---|---|
| Bovine Mastitis | Several outbreaks with hundreds of animals involved | Likely direct inoculation related to contaminated equipment | Stopped with infection control practices | (70;118) |
| Vancouver/ NW USA humans/animals | Hundreds with disease | Ecologic change with recombinant strain and improved fungal fitness | Ongoing,clinicians aware of disease in area | (69) |
| Worldwide with HIV pandemic | Millions with disease | Severe immunosuppression and reactivation disease | Continues as HIV pandemic remains | ((A):109) |
Table 3: Monographs, Reviews or Books with Critical Description of this Yeast Through History.
| Date | Authors | Title | Focus | Ref. |
|---|---|---|---|---|
| 1916 | Stoddard/Cutler | Torula infection in man | Description of CNS Cryptococcosis. | (148) |
| 1956 | Littman/Zimmerman | Cryptococcosis | History clinical description prior to effective treatment | (79) |
| 1971 | Al-Doory | A bibliography of Cryptococcosis | Listing of published papers on cryptococcosis | (3) |
| 1995 | Perfect/Mitchell | Cryptococcosis over the first century | Cryptococcosis with an emphasis on AIDS era | (95) |
| 1997 | Drouhet | Milestones in the history of cryptococcus and cryptococcosis | Historical view of cryptococcus | (36) |
| 1998 | Casadevall/Perfect | Cryptococcus neoformans | Greater than 500 page book devoted in depth to cryptococcosis | ((A):25) |
Table 4. Predisposing Factors of Cryptococcosis
(A):
| HIV Infection |
|---|
| Corticosteroids (? 20 mg of prednisone) |
| Solid organ transplantationa |
| Malignanciesa (ie, Hodgkin’s disease, lymphomas, chronic |
| lymphocytic leukemia) |
| CD4+ T-cell lymphopenia |
| Connective tissue diseases or immunologic diseasesa (ie. sarcoidosis, systemic lupus erythematosus, rheumatoid arthritis, hyper lgM syndrome of hyper lgE syndrome) |
| Monoclonal antibodies (etanercept, infliximab, alemtuzumab) |
| Diabetes mellitus |
| Chronic pulmonary diseases or lung cancer |
| Renal failure or peritoneal dialysis |
| Cirrhosis |
| Pregnancy |
| aImmunosuppressive therapies add to the risk. |
| Adapted from Cryptococcus neoformas. Casadevall A. Perfect JR. ASM Press. ((A):26) |
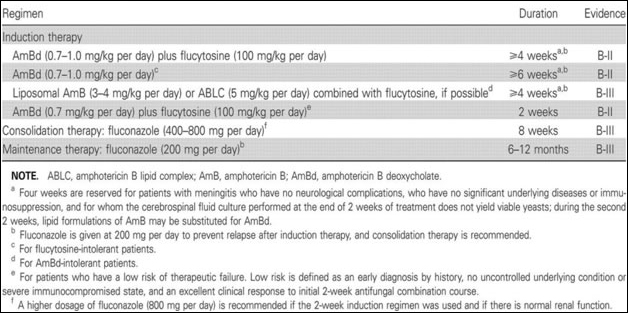
Table 5. Antifungal Treatment Recommendations for Cryptococcal Meningoencephalitis in Human Immunodeficiency Virus – InfectedIndividualse
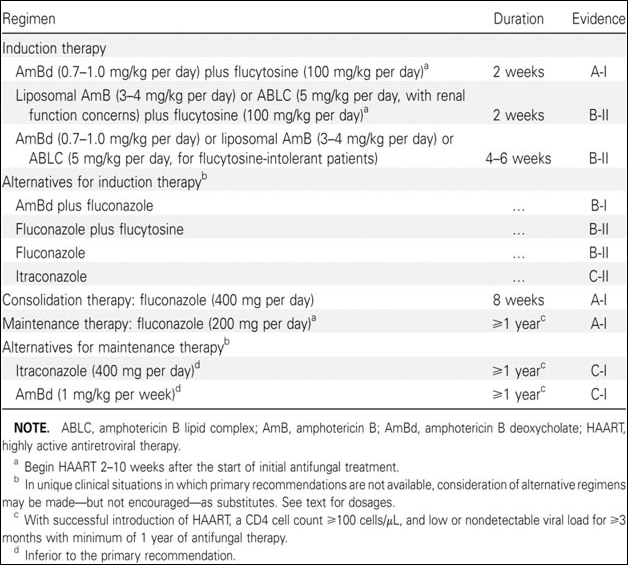 |
| e2010 IDSA Cryptococcal Guidelines ((A):112) |
Table 6. Antifungal Treatment Recommendations for Cryptococcal Meningoencephalitis in Transplant Recipients g
 |
| e2010 IDSA Cryptococcal Guidelines ((A):112) |
Table7. Antifungal Treatment Recommendations for Cryptococcal Meningoencephalitis in Non–Human Immunodeficiency Virus–Infected and Nontransplant Patients g
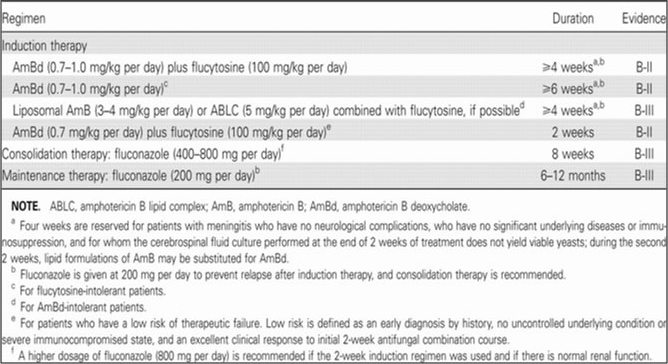 |
| e2010 IDSA Cryptococcal Guidelines ((A):112) |
Table 8. Antifungal Treatment Recommendations for Nonmeningeal Cryptococcosis b
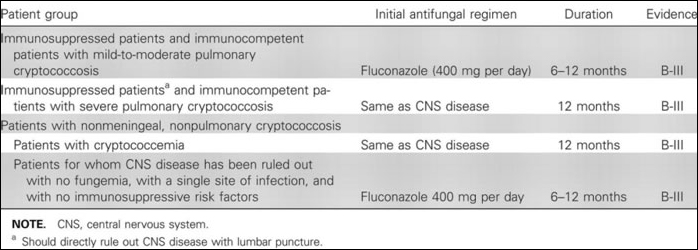 |
| e2010 IDSA Cryptococcal Guidelines ((A):112) |