Title: A Case of Potential Sexual Transmission of Trichophyton indotineae, an Emerging Drug-resistant Dermatophyte
Submitted by: Stephanie Spivack, MD (1); Mahmoud Ghannoum (2)
Institution:
- Temple University Hospital, Philadelphia PA
- Center for Medical Mycology of the University Hospitals Cleveland Medical Center, Cleveland OH
Email: Stephanie.spivack@tuhs.temple.edu
Date Submitted: May 9, 2024
History: A 26-year-old healthy female presented to Infectious Diseases for evaluation of a rash that had been present for over one year. The rash first started when she traveled to Bangladesh and had sexual intercourse with a male partner who had a rash on his genitals and buttocks. Shortly afterward, she developed similar lesions on her inner thigh, vulva, and buttocks that were very itchy. She was evaluated by a dermatologist upon returning to the United States and received a variety of treatments, including mometasone ointment for suspected contact dermatitis, a prednisone taper pack, diphenhydramine, topical ecoazole, topical ketoconazole, oral terbinafine (250 mg/day for 2 weeks), and fluconazole (150 mg/week to 200 mg/day for >20 cumulative weeks). The reported lesions did not significantly improve, and corticosteroids worsened the condition. She also reported that a new male sexual partner also developed similar lesions.
Physical Examination:
General: well-appearing female in no distress
Dermatologic: Notable for an annular, scaling, hyper-pigmented eruption on the patient’s buttocks involving the intergluteal cleft and 3 small hyper-pigmented areas on the mons pubis.
Laboratory Examination:
A complete blood count and comprehensive metabolic panel were within normal limits. An HIV test was non-reactive. Hepatitis B and C serologies were negative.
A punch biopsy of the thigh was performed by dermatology and was positive for hyphae by periodic acid-Schiff stain, consistent with dermatophytosis.
A fungal culture from a skin scraping had no growth at 4 weeks.
Question 1: What are probable/possible diagnoses?
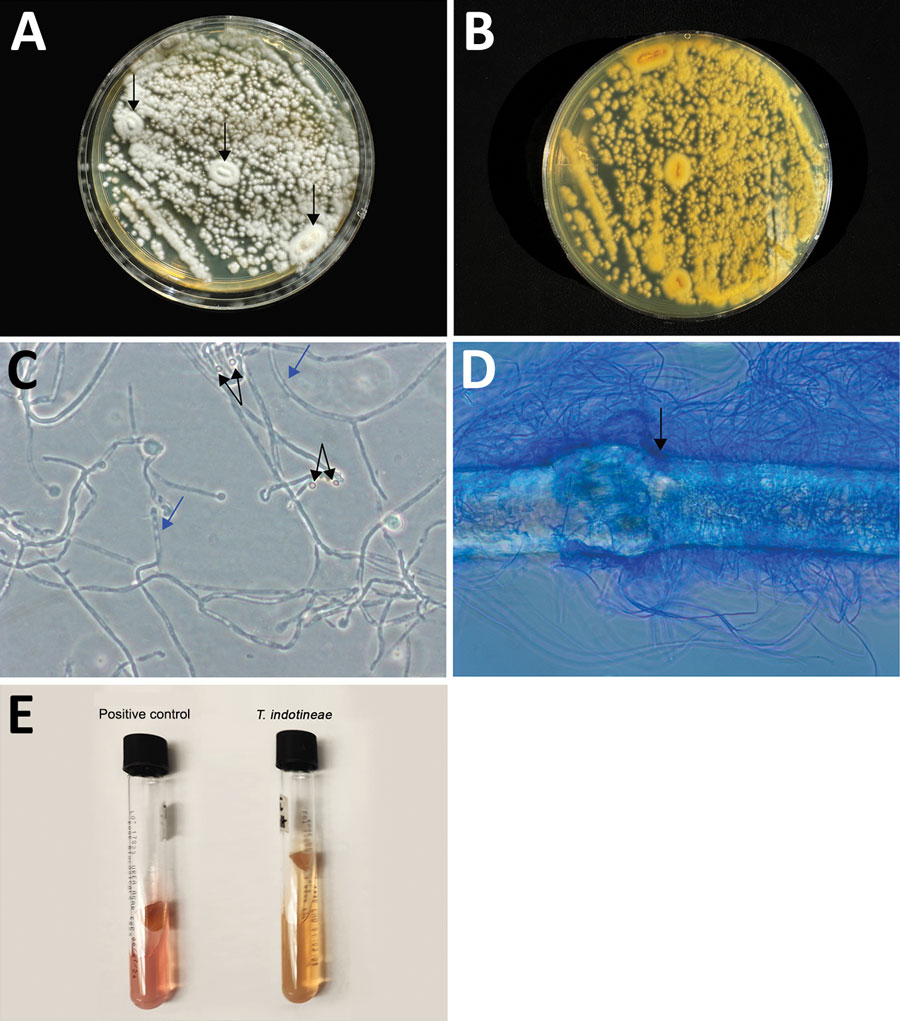
Microbiology/Diagnostic Tests Performed: A skin scraping from the gluteal region was collected and sent for fungal culture and advanced mycologic testing at the Center for Medical Mycology of the University Hospitals Cleveland Medical Center (Cleveland, OH, USA). Macroscopic and microscopic morphology (Figure 1) and broth microdilution antifungal susceptibility testing demonstrated MICs of 16 μg/mL for terbinafine, 16 μg/mL for fluconazole, 0.016 μg/mL for itraconazole, and ≤0.031 μg/mL for efinaconazole.
Although breakpoints do not exist for dermatophytes, MIC ≥0.5 μg/mL for terbinafine has been correlated with resistance-conferring gene mutations. The isolate was initially identified as T. interdigitale. Given concern for T. indotineae infection, a BLAST search was then performed which identified the isolate as T. indotineae.
Final Diagnosis: Tinea genitalis due to Trichophyton indotineae
Question 2: What treatment is recommended in the care of this patient?
Treatment: Itraconazole is the recommended treatment. This fungus is typically resistant to first-line agents including terbinafine.
Outcome: The patient initially had improvement of her symptoms after a 7-day course of itraconazole, but symptoms recurred about 6 weeks after treatment was completed. She was treated with a 14-day course of itraconazole and had complete resolution of her symptoms with no recurrence at 3 months.
Discussion: Tinea, commonly known as “ringworm,” is an infection with dermatophytes including Trichophyton, Microsporum, and Epidermophyton species. Visual inspection cannot reliably distinguish dermatophytosis from other skin conditions such as contact dermatitis, but corticosteroids can exacerbate dermatophytosis. Clinicians should suspect T. indotineae in a person with dermatophytosis that does not improve with terbinafine.
In South Asia, an outbreak of drug-resistant tinea was identified. The organisms causing this were initially identified as T. mentagrophytes ITS genotype VIII. However, after additional genomic studies, these strains were found to be distinct from T. mentagrophytes and were reclassified as a new species, T. indotineae. T. indotineae exhibits resistance to commonly used antifungals, particularly terbinafine. So far, a handful of cases have been reported in the United States. Most cases occurred after travel to South Asia, but there has been at least one reported case in a person with no international travel.
As this case highlights, it is difficult to diagnose T. indotineae by standard methods. Clinicians who suspect antifungal-resistant dermatophytosis can contact their state and local health departments for assistance
(https://www.cdc.gov/publichealthgateway/healthdirectories/index.html).
Public health officials concerned about potential cases of antifungal-resistant ringworm or unusual clusters of cases can email FungalOutbreaks@cdc.gov for assistance with recommendations and testing.
Clinicians can request consultation for the evaluation and management of challenging STI cases from the National Network of STD Clinical Prevention Training Centers (NNPTC) STD Clinical Consultation Network, which is supported by the CDC Division of STD Prevention, at https://www.stdccn.org.
Itraconazole is the preferred treatment for T. indotineae, however, there are issues with itraconazole for clinicians to be aware of. These include cost; issues with absorption especially when given with acid suppressing medications; drug-drug interactions particularly with CYP3A4 substrates; hepatotoxicity; and cardiac effects including QTc prolongation and heart failure exacerbation.
Key References:
- Caplan AS, Chaturvedi S, Zhu Y, Todd GC, Yin L, Lopez A, et al. Notes from the field: first reported US cases of tinea caused by Trichophyton indotineae—New York City, December 2021–March 2023. MMWR Morb Mortal Wkly Rep. 2023;72:536–7.
- Uhrlaß S, Verma SB, Gräser Y, Rezaei-Matehkolaei A, Hatami M, Schaller M, et al. Trichophyton indotineae—an emerging pathogen causing recalcitrant dermatophytoses in India and worldwide: a multidimensional perspective. J Fungi (Basel). 2022;8:757.
- Cañete-Gibas CF, Mele J, Patterson HP, Sanders CJ, Ferrer D, Garcia V, et al. Terbinafine-resistant dermatophytes and the presence of Trichophyton indotineae in North America. J Clin Microbiol. 2023;61:e0056223.
- Luchsinger I, Bosshard PP, Kasper RS, Reinhardt D, Lautenschlager S. Tinea genitalis: a new entity of sexually transmitted infection? Case series and review of the literature. Sex Transm Infect. 2015;91:493–6.