(described by Negroni and Fischer in 1943)
Taxonomic classification
Kingdom: Fungi
Phylum: Ascomycota
Class: Euascomycetes
Order: Microascales
Family: Microascaceae
Genus: Pseudallescheria

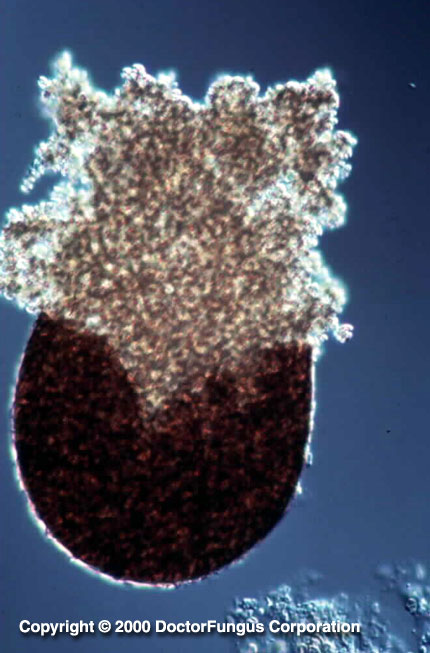
A globose and black cleistothecium that forms beneath the agar is typical of Pseudallescheria boydii

Scedosporium apiospermum is one of the asexual forms of Pseudallescheria boydii
Description and Natural Habitats
Pseudallescheria is a filamentous fungus that is found worldwide. It has so far been isolated from soil [2194], sewage, contaminated water, and the manure of farm animals. It is an emerging opportunistic pathogen and can cause various infections in humans. Pseudallescheria boydii is the telemorph of Scedosporium apiospermum and Graphium eumorphum. It is a homothallic fungus.
Species
The genus Pseudallescheria contains a single species; Pseudallescheria boydii. See the list of obsolete names and synonyms for Pseudallescheria sp.
Pathogenicity and Clinical Significance
The infections caused by Pseudallescheria boydii are occasionally and wholely referred to as pseudallescheriasis. The affected host is commonly immunosupressed due to various reasons, such as hematological malignancies, organ transplantation or AIDS [62, 755, 908, 1565, 1736, 2045]. Pseudallescheria boydii is among the causative agents of white grain mycetoma [724, 2166]. The infection is usually acquired via contact with soil and follows a minor trauma. In addition to mycetoma, Pseudallescheria boydii is well-known to cause infections in various organs and systems of the body. These include cutaneous infections [235, 1316, 1550], sinusitis [905, 929, 959, 1086, 2003, 2042, 2089, 2146, 2386], keratitis [263, 1541, 1979], lymphadenitis [1194], endophthalmitis [302, 401, 1498, 1786], meningoencephalitis [227, 637, 807, 1077, 1741, 1841], brain abscess [227, 640, 962, 963, 1756, 2062], endocarditis [1865, 2405], pneumonia [1653], lung abscess [1526], pulmonary fungus ball [2082, 2148], allergic bronchopulmonary fungal disease [1286], bursitis [752], arthritis [562, 821, 1802], osteomyelitis [724, 1084], urethritis [2018], and disseminated infections [1503, 1789, 2062]. Disseminated infections are often fatal if not treated. Cerebral infections are commonly encountered as a complication in near-drowning patients [962, 1184].
Pseudallescheria boydii has also been reported to cause keratitis [2115], abdominal eumycotic mycetoma and disseminated infections [49, 200, 2351] in dogs, and keratitis [777] and eumycotic mycetoma [1483] in horse.
Macroscopic Features
Colonies of Pseudallescheria boydii grow rapidly at 25°C. The texture is wooly to cottony. From the front, the color is initially white and later becomes dark gray or smoky brown. From the reverse, it is pale with brownish black zones [531, 1295, 2144, 2202].
Microscopic Features
Cleistothecia, asci, and ascospores are visualized in the sexual stage. Strains isolated from clinical samples rarely produce the sexual reproductive structures and an incubation of 2 to 3 weeks is required for formation of cleistothecia. Cleistothecium (50 to 250 µm in diameter) is a round, closed, brown, multicellular, sexual fruiting body. It bears asci and ascospores inside. The cleistothecium of Pseudallescheria boydii does not have appandages or ostioles. At maturation, the cleistothecium bursts and releases the asci that are filled with ascospores. Asci are subglobose to globose and bear 8 ascospores inside. Ascus walls readily dissolve to release the ascospores. Ascospores are unicellular, ovoid to ellipsoidal, smooth, and pale yellow brown to copper in color.
In the asexual stage (Scedosporium apiospermum or Graphium eumorphum), the asexual reproductive structures; septate hyaline hyphae (2-4 µm in diameter), conidiophores and (annello)conidia are produced. The conidiophores of Scedosporium apiospermum are simple while those of Graphium eumorphum are long, erect, narrow, and cemented together forming synnemata (the erect structure consisting of united conidiophores). Conidia (4-7 x 5-12 µm) of both Scedosporium apiospermum and Graphium eumorphum are unicellular and oval in shape. They are typically truncate at their base. The conidia of Scedosporium apiospermum are often formed singly on the conidiophores while those of Graphium eumorphum are arranged in clusters at the apices of each synnema. Scedosporium, Graphium or both forms may be present in the same isolate [531, 1295, 2144, 2202].
Histopathologic Features
(Mats of) septate hyphae may be observed in the infected tissues [2061, 2148]. See also our histopathology page.
Compare to
Blastomyces dermatitidis
Petriella
Phoma spp.
Sporothrix schenckii
Pseudallescheria differs from Blastomyces dermatitidis and Sporothrix schenckii by not converting to a yeast phase at 37°C. It differs from Petriella by forming non-ostiolate cleistothecia.
Laboratory Precautions
No special precautions other than general laboratory precautions are required.
Susceptibility
Miconazole [1511],
itraconazole [1511],
voriconazole [1152, 1493, 1511], posaconazole [1434, 1511], ravuconazole, the novel triazole, UR-9825 [386, 1511], echinocandins, such as caspofungin [1780], and sordarins [1040] are active in vitro against Scedosporium apiospermum. Interestingly, a chemically modified tetracycline, CMT-3 also proved to be active in vitro against Pseudallescheria boydii as well as some other fungal genera [1358].
MICs of amphotericin B, nystatin, liposomal nystatin, and terbinafine against clinical Scedosporium apiospermum isolates are often high [1511, 1973]. Promisingly, terbinafine was found to be synergistic with azoles [1990] against this fungus.
For MICs of various antifungal drugs for Pseudallescheria boydii, see our N/A(L):susceptibility database.
Pseudallescheria boydii is often resistant to treatment with amphotericin B [2353]. Some patients have successfully been treated with ketoconazole [799, 1526, 2166, 2438], itraconazole [860, 1194, 1456, 1653, 1802, 2169], posaconazole [1515], and voriconazole [1598, 1633, 1841]. Topical miconazole [1979] and natamycin have proven to be effective in cases with keratitis [1541]. Concomitant surgical intervention may be required in some cases, such as those with sinusitis [905, 929], keratitis [1541] or brain abscess [1515, 1633].