Title:
When a Colon Mass Is Not Cancer: Gastrointestinal Basidiobolomycosis With Hepatic Involvement
Submitted by:
Taghrid Taha, MD, Saman Nematollahi, MD, William Lainhart, PhD, D(ABMM)
Institution:
Banner Health-University of Arizona College of Medicine – Tucson
Email:
taghreedtarek111@gmail.com
Date Submitted:
May 2026
History:
A 56-year-old male presented to the emergency department with progressive left-sided abdominal pain for 3 weeks. The pain was sharp, rated 6/10, worsened with bowel movements and palpation, and had no alleviating factors. He had previously seen his primary care physician and completed a course of metronidazole without improvement. He endorsed bright red blood mixed with stool and low-grade fevers over the preceding two days.
Past medical history included hypertension, hyperlipidemia, and anxiety. Colonoscopy performed three months earlier demonstrated diverticulosis, internal hemorrhoids, and a 3 mm colon polyp that was removed. He denied tobacco, alcohol, or illicit drug use. Family history was notable for ulcerative colitis in his mother.
Additional epidemiologic history revealed prior residence in Austria approximately 30 years earlier, travel to Cabo, Utah, Seattle, Tennessee, and North Carolina, remote hunting exposure with elk meat ingestion, horse meat ingestion while living in Austria, and frequent restaurant food consumption including tacos and various meat products. He denied pet ownership, although his daughter owned dogs with whom he had regular contact.
Physical Examination:
- Temperature: 38.2°C
- Heart rate: 115 bpm
- Respiratory rate: 18/min
- Blood pressure: 137/90 mmHg
- Oxygen saturation: 97% on room air
The patient appeared mildly diaphoretic and had diffuse abdominal tenderness on palpation. The remainder of the physical examination was unremarkable.
Laboratory Examination:
- WBC: 16 ×10⁹/L
- Neutrophils: 11.9 ×10⁹/L
- Eosinophils: 1.4 ×10⁹/L
- Monocytes: 1.6 ×10⁹/L
- ALT: 87 U/L
- AST: 24 U/L
- Alkaline phosphatase: 250 U/L
Microbiologic workup revealed:
- Blood cultures: negative
- Colon tissue cultures: negative
- GI panel: negative
- Clostridioides difficile testing: negative
- HIV serology: negative
- Hepatitis B/C serologies: negative
- Stool ova and parasite examination: negative
- Coccidioidal serology: negative
- Serum β-D-glucan: 84 pg/mL
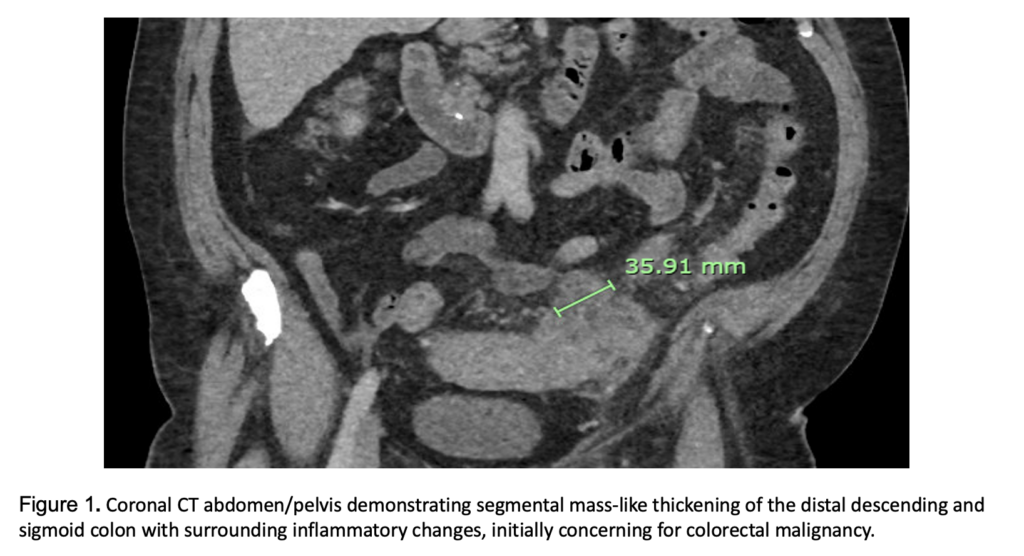
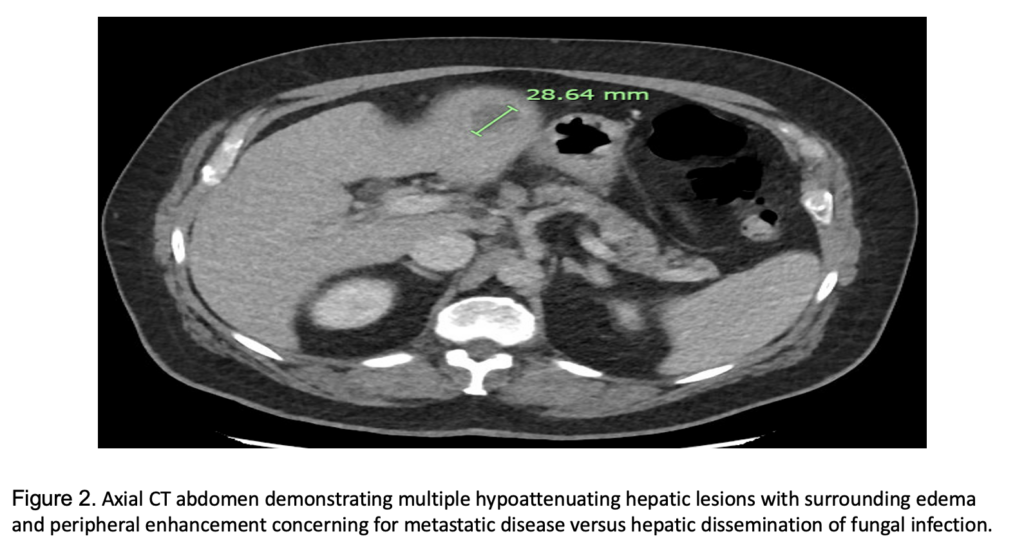
CT abdomen/pelvis demonstrated segmental thickening of the distal descending/sigmoid colon with multifocal mass-like outpouching and moderate pericolonic inflammatory changes. Multiple low-attenuation hepatic lesions with surrounding edema and peripheral enhancement were identified, concerning for metastatic disease. Enlarged mesenteric and para-aortic lymph nodes were also noted [Figure 1,2].
Blood cultures were obtained, and empiric piperacillin-tazobactam was initiated. Gastroenterology and Oncology services were consulted for concern of gastrointestinal malignancy with liver metastases.
Question 1: What are probable/possible diagnoses?
The initial differential diagnosis included:
- Colorectal malignancy with hepatic metastases
- Inflammatory bowel disease
- Invasive fungal infection
- Intestinal tuberculosis
- Hepatocellular carcinoma
Microbiology/Diagnostic Tests Performed:
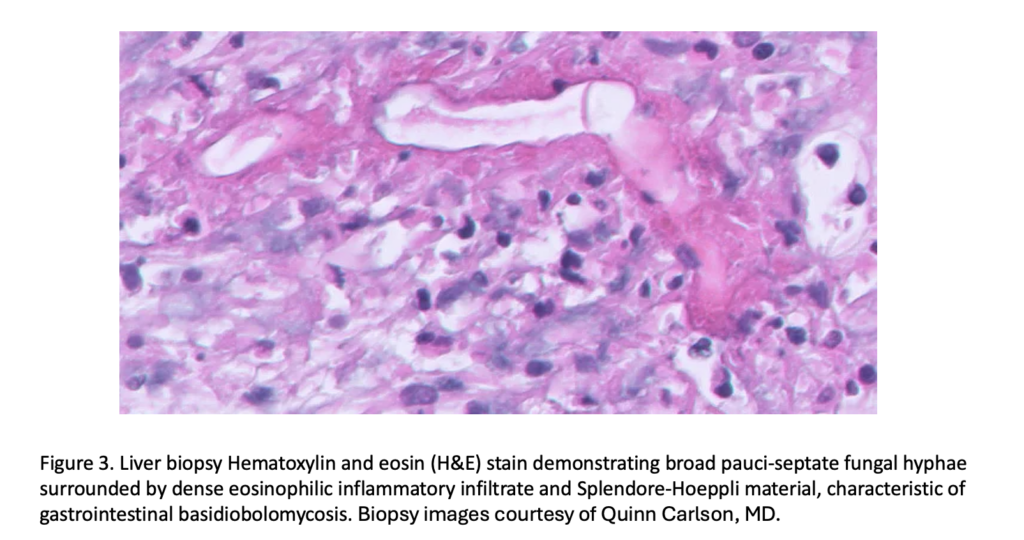
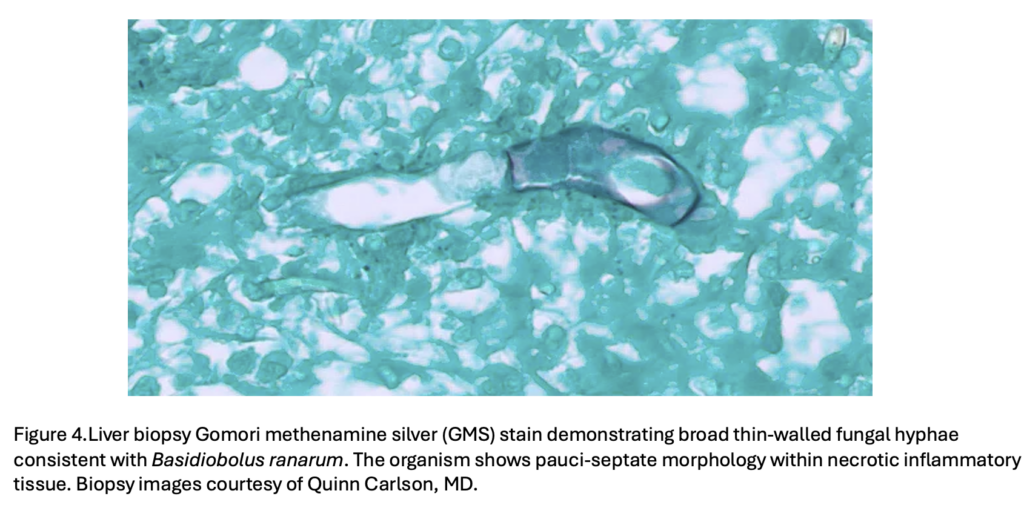
Liver biopsy demonstrated necrotic tissue with abscess formation and abundant eosinophils. Histopathology revealed broad septate thin-walled fungal hyphae surrounded by eosinophilic material consistent with the Splendore-Hoeppli phenomenon. GMS stain was weakly positive for fungal hyphae. [Figure 3,4]. PCR performed on tissue confirmed Basidiobolus ranarum.
Final Diagnosis:Gastrointestinal basidiobolomycosis with hepatic involvement due to Basidiobolus ranarum.
Question 2: What treatment is recommended in the care of this patient?
Recommended management includes combined surgical intervention and prolonged systemic antifungal therapy. Amphotericin B formulations combined with azole therapy, such as itraconazole or voriconazole, are commonly used. Surgical resection is frequently required in gastrointestinal disease due to mass-forming lesions and concern for malignancy.
Treatment:
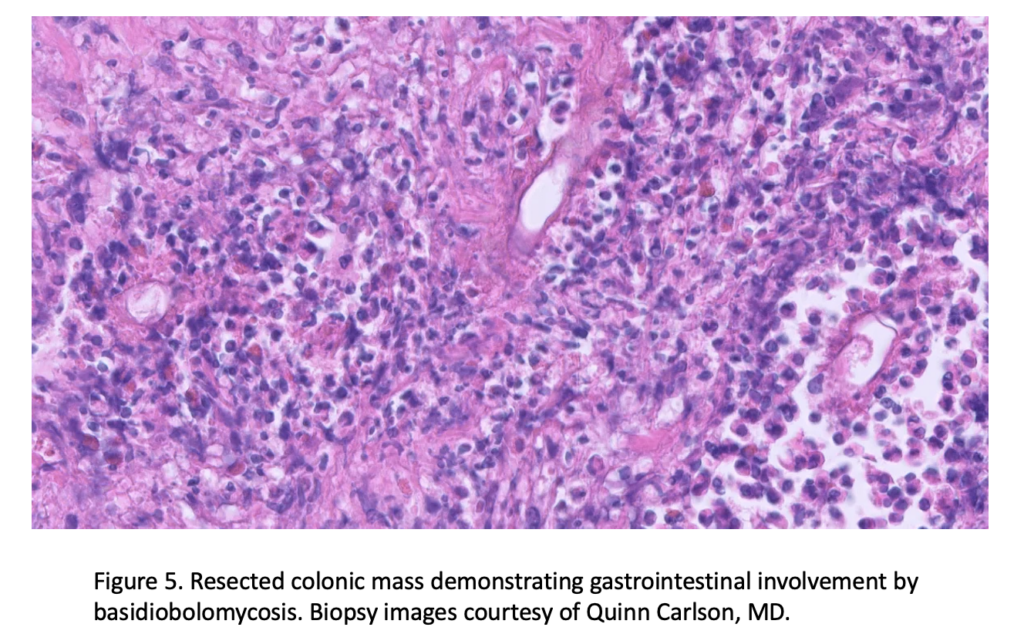
The patient underwent surgical resection of the involved colonic lesion with pathology demonstrating involvement by basidiobolomycosis [Figure 5] and received Amphotericin B and voriconazole.
Outcome:
The patient demonstrated clinical improvement following combined medical and surgical management.
Discussion:
Basidiobolomycosis is a rare, chronic granulomatous fungal infection caused by Basidiobolus ranarum, a saprophytic fungus from the order Entomophthorales. Unlike invasive mucormycosis, basidiobolomycosis generally affects immunocompetent individuals. Basidiobolus ranarum is found in soil, decaying vegetation, and the gastrointestinal tracts of amphibians, reptiles, fish, and bats. Gastrointestinal basidiobolomycosis (GIB) is believed to result from ingestion of contaminated material. [1–2]
Although traditionally described in tropical and subtropical regions, GIB has increasingly been reported in the Southwestern United States, especially in Arizona. [3] Clinical features are nonspecific and often resemble inflammatory bowel disease or intra-abdominal malignancy. Common symptoms include abdominal pain, fever, abdominal mass, hematochezia, hepatic lesions, and peripheral eosinophilia. [2–4]
In the presented case, the patient was initially thought to have metastatic colorectal carcinoma, as imaging showed mass-like colonic thickening with hepatic lesions and lymphadenopathy. However, the presence of marked eosinophilia and characteristic histopathologic features suggested an alternative diagnosis. Histopathology is the cornerstone of GIB diagnosis and typically demonstrates broad, thin-walled, septate or pauciseptate hyphae surrounded by eosinophilic material (Splendore-Hoeppli phenomenon) within granulomatous eosinophilic inflammation. [1,2] Peripheral eosinophilia, as seen in this case, is a major diagnostic clue and is reported in most patients with GIB. [4]
Culture is considered the diagnostic gold standard but has limited sensitivity, with positive cultures reported in only 15–25% of cases. [3] Molecular methods such as PCR are increasingly useful when cultures are negative or tissue samples are limited. In this case, PCR confirmed Basidiobolus ranarum despite negative routine cultures.
The differential diagnosis includes colorectal carcinoma, Crohn’s disease, eosinophilic gastroenteritis, intestinal tuberculosis, and invasive fungal infections such as mucormycosis and aspergillosis. Distinguishing basidiobolomycosis from mucormycosis is particularly important because mucormycosis typically affects immunocompromised patients and is characterized by angioinvasion and tissue infarction, in contrast to the eosinophilic granulomatous inflammation seen in GIB. [5]
No standardized treatment guidelines exist for GIB due to its rarity. Management is tailored to disease severity and the site of involvement. Itraconazole is commonly used for subcutaneous disease, while voriconazole has shown favorable outcomes in gastrointestinal disease, with one large series reporting an 83% response rate to voriconazole monotherapy. Severe or disseminated cases may necessitate amphotericin B formulations. Surgical intervention is often required in GIB, and the best outcomes are achieved with a combination of surgical resection and prolonged antifungal therapy. [4,6-7] Early recognition and initiation of treatment are crucial, as delayed diagnosis can result in widespread dissemination to the liver, pancreas, retroperitoneum, or other abdominal organs.
Key References:
- Vikram HR, Smilack JD, Leighton JA, Crowell MD, De Petris G. Emergence of gastrointestinal basidiobolomycosis in the United States, with a review of worldwide cases. Clin Infect Dis. 2012;54(12):1685-1691. PMID: 22441651.
- Geramizadeh B, Heidari M, Shekarkhar G. Gastrointestinal basidiobolomycosis: a review of 14 cases. Iran J Med Sci. 2015;40(5):373-379. PMID: 25821287.
- Lyon GM, Smilack JD, Komatsu KK, et al. Gastrointestinal basidiobolomycosis in Arizona: clinical and epidemiological characteristics and review of the literature. Clin Infect Dis. 2001;32(10):1448-1455. PMID: 11317246.
- Al Jarie A, Al Azraki T, Al Mohsen I, et al. Basidiobolomycosis: case series and review of literature. Pediatr Infect Dis J. 2003;22(11):1007-1014. PMID: 14614376.
- Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis. Lancet Infect Dis. 2019;19(12):e405-e421. PMID: 31699664
- Pouladfar G, Jahangiri S, Shahpar A, et al. Navigating treatment for basidiobolomycosis: a qualitative review of 24 cases. BMC Infect Dis. 2024;24(1):816. PMID: 39134962
- Rathore M, Sharma S, et al. Subcutaneous basidiobolomycosis masquerading as cellulitis on the forearm of an elderly woman. Cureus. 2024;16(8): e67874. PMID: 40262576
Images and Figures:
Figure 1 Coronal CT abdomen/pelvis demonstrating segmental mass-like thickening of the distal descending and sigmoid colon.
Figure 2 Axial CT abdomen demonstrating multiple hypoattenuating hepatic lesions.
Figure 3 Liver biopsy Hematoxylin and eosin (H&E) stain demonstrating broad pauci-septate fungal hyphae surrounded by dense eosinophilic inflammatory infiltrate and Splendore-Hoeppli material.
Figure 4 Liver biopsy Gomori methenamine silver (GMS) stain demonstrating broad thin-walled fungal hyphae consistent with Basidiobolus ranarum.
Figure 5 Resected colonic mass demonstrating gastrointestinal involvement by basidiobolomycosis.