Synonyms
Cerebral chromomycosis, chromoblastomycosis (in part), chromomycosis (in part), cladosporiosis, phaeomycotic cyst, phaeosporotrichosis, subcutaneous mycotic cyst.
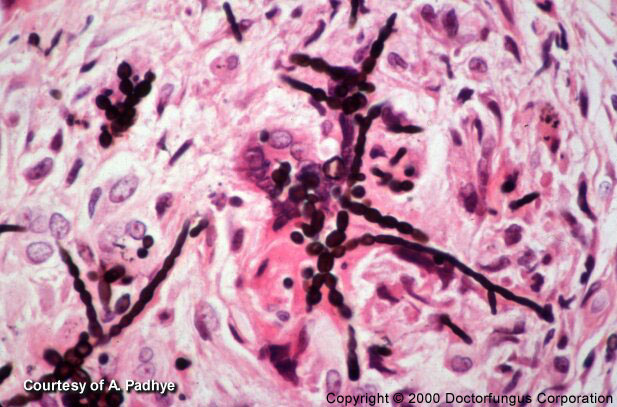
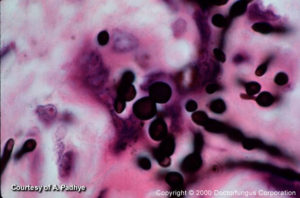
H and E stain of tissue with Exophiala spinifera
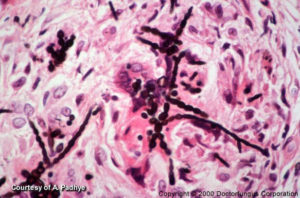
H and E with GMS stain tissue with Exophiala spinifera

Phaeohyphomycosis of arm caused by Exserohilum rostratum

Phaeohyphomycosis of arm caused by Exserohilum rostratum.
Definition
Phaeohyphomycosis consists of a group of mycotic infections characterized by the presence of dematiaceous (dark-walled) septate hyphae and sometimes yeast or a combination of both in tissue. The hyphae may be short to elongate, distorted or swollen (toruloid hyphae), regularly shaped, or any combination of the above. The yeast when present will be variable in size and most of the time will show budding. The yeast should not be confused with the sclerotic Medler cells seen with the agents of chromoblastomycosis in subcutaneous tissue, although there are case reports of Wangiella (Exophiala) dermatitidis and Exophiala jeanselmei producing a combination of hyphae, yeast, and sclerotic cells from deep infections that otherwise could not be classified as chromoblastomycosis. Infections of the eyes and skin by the black fungi could also be classified as phaeohyphomycosis [9, 449, 700, 726, 1927, 2075, 2184].
Forms of the disease
| CATEGORIES | VARIETIES | COMMENTS | REFERENCES |
|---|---|---|---|
| Superficial | Black piedrae Skin infections | Infection only involves the stratum corneum.
Minimal if any tissue response. In hairy areas, the fungi grow around the hair shaft |
[700] |
| Cutaneous | Dermatomycosis
Onychomycosis |
Infection affects keratinized tissue and produces extensive destruction | [726] |
| Corneal | Mycotic keratitis | Lesions are classically produced by traumatic inoculation of the etiologic agent | [9, 73, 74, 1847] |
| Subcutaneous | Infection is produced by traumatic inoculation of the etiologic agent
Abscess formation is frequent |
[342, 449, 478, 1701, 2184] | |
| Respiratory tract | Nasal
Sinus Pneumoniae |
Dark lesion on the septum is a common presentation; sinusitis is associated with allergic rhinitis, polyps and/or some form of immunosuppression | [1239, 1487, 1873, 1927, 2127, 2482] |
| Others | Brain
Peritoneal cavity Bone |
Carries a poor prognosis
Associated with peritoneal dialysis Usually follows a traumatic injury |
[9, 416, 1411, 1608, 1706, 1847, 2075] |
Prognosis and therapy
Most cases of phaeohyphomycosis can be controlled by surgical excision and chemotherapy. Amphotericin B and 5-fluorocytosine or Itraconazole are the drugs of choice. Invasion of the brain or bone has a grave prognosis [9, 449, 700, 2344].
Histopathology
The histopathology is extremely varied, ranging from tissue reactions associated with walled abscesses to active tissue invasion by hyphae. Most of the time the hyphae will stain positive for the Fontana-Masson or other melanin stains.
Laboratory
Direct examination
Clinical materials such as pus and tissue are mounted in 10% KOH for examination. The dematiaceous nature of the hyphal elements is a key characteristic for the diagnosis of phaehyphomycosis. The hyphae may be regular in shape or variable. In some cases special stains such as Fontana may help in the diagnosis of the disease.
Isolation
The specimens are inoculated onto Inhibitory Mould Agar and/or Saboraud Dextrose Agar and a medium containing cycloheximide and then incubated at 30°C. Many of the etiologic agents of phaeohyphomycosis are sensitive to cycloheximide. The cultures are discarded as negative in 4 weeks. The isolated fungus must be compatible with the clinical disease and tissue morphology (that is, dematiaceous) before it can be concluded that it is the etiologic agent involved.
Mycology (principal fungi)
- N/A(L):Cladophialophora bantiana
- N/A(L):Curvularia spp.
- N/A(L):Bipolaris spp.
- Exserohilum spp.
- N/A(L):Exophiala jeanselmei
- N/A(L):Scedosporium prolificans
- Ochroconis gallopava
- Coniothyrium fuckelii
- N/A(L):Phialophora parasitica
- N/A(L):Phialophora repens
- N/A(L):Wangiella dermatitidis
- Lasiodiplodia theobromae
Natural habitat
Ubiquitous
Susceptibility Testing
Standardized testing procedures are not available. Microbiological resistance has not been demonstrated.