(described by Ehrenberg ex Corda in 1838)
Taxonomic classification
Kingdom: Fungi
Phylum: Zygomycota
Order: Mucorales
Family: Mucoraceae
Genus: Rhizopus
Description and Natural Habitats
Rhizopus is a cosmopolitan filamentous fungus found in soil, decaying fruit and vegetables, animal feces, and old bread. While Rhizopus spp. are common contaminants, they are also occasional causes of serious (and often fatal) infections in humans. Some species are plant pathogens [531, 1295, 2144, 2202].
Species
The genus Rhizopus contains several species. The most common ones are Rhizopus arrhizus, Rhizopus azygosporus, Rhizopus microsporus, Rhizopus schipperae, and Rhizopus stolonifer.
Some morphological features, such as the length of rhizoids and sporangiophores, the diameter of sporangia, the shape of columellae, and the size, shape and surface texture of sporangiospores aid in differentiation of Rhizopus species from eachother. Maximum growth temperature also varies from one species to other [1295].
See the list of obsolete names and synonyms for older names of Rhizopus spp.
Pathogenicity and Clinical Significance
Rhizopus spp. are among the fungi causing the group of infections referred to as zygomycosis. Although the term mucormycosis has often been used for this syndrome, zygomycosis is now the preferred term for this angio-invasive disease. Rhizopus arrhizus is the most common cause of zygomycosis [408] and is followed by Rhizopus microsporus var. rhizopodiformis.
Zygomycosis includes mucocutaneous, rhinocerebral, genitourinary, gastrointestinal, pulmonary, and disseminated infections [104, 408, 502, 696, 963, 1318, 2042, 2220]. Diabetic ketoacidosis and immunosuppression due to various reasons, such as organ transplantation are the most frequent predisposing factors [408, 696, 910, 1731]. Desferoxamine treatment, renal failure, extensive burns, trauma, and intravenous drug use may also predispose to development of zygomycosis [1918]. While heatstroke has been described as a risk factor for disseminated zygomycosis [104], contaminated adhesive tapes and wooden tongue depressors have been reported to lead to nosocomial outbreaks of zygomycosis [812]. Vascular invasion that causes necrosis of the infected tissue, and perineural invasion are the most frustrating features of these infections [763]. Zygomycosis is frequently fatal.
Macroscopic Features
Colonies of Rhizopus grow very rapidly, fill the Petri dish, and mature in 4 days. The texture is typically cotton-candy like. From the front, the color of the colony is white initially and turns grey to yellowish brown in time. The reverse is white to pale. Pathogenic species of Rhizopus can grow well at 37°C [531, 1295, 2144, 2202].
Microscopic Features
Nonseptate or sparsely septate broad hyphae (6-15 µm in diameter), sporangiophores, rhizoids (root-like hyphae), sporangia, and sporangiospores are visualized. Sporangiophores are brown in color and usually unbranched. They can be solitary or form clusters. Rhizoids are located at the point where the stolons and sporangiophores meet. Sporangia (40-350 µm in diameter) are located at the tip of the sporangiophores. They are round with flattened bases. Apophysis is absent or rarely apparent and columellae are hemispherical. Sporangiospores (4-11 µm in diameter) are unicellular, round to ovoid in shape, hyaline to brown in color, and smooth or striated in texture [1295, 2144].
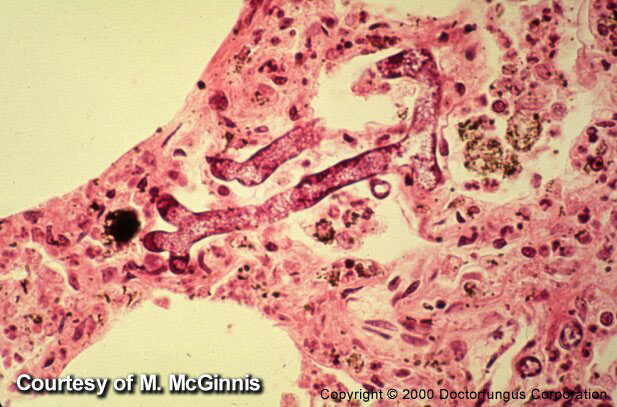
Histopathologic Features
Broad, thin-walled, hyaline, often aseptate or sparsely septate hyphae are observed in the infected tissues. The contours of the hyphae are typically non-parallel and branches are irregular. Invasion of blood vessels is noteworthy [462, 763]. See also our histopathology page.
Compare to
Rhizopus spp. must be differentiated from the other genera included in the phylum Zygomycota:
Absidia
Apophysomyces
Rhizomucor
Mucor
Mortierella
The features that help in differentiation of these genera are summarized in the table below [531, 1295, 2144, 2202].
| Genus | Best growth | Sporangiophore | Apophysis | Columella | Sporangium | Rhizoid | Stylospore |
|---|---|---|---|---|---|---|---|
| Absidia | 45°C | Branched, hyaline | Conical, not prominent | Dome-shaped | Pear-shaped | +, but usually indistinct | – |
|
Apophysomyces
|
>42°C | Usually unbranched, grayish-brown | Bell-shaped, not prominent | Usually dome-shaped, rarely elongated | Pear-shaped | + | – |
| Mortierella | 40°C | Branched, hyaline | – | – | Spherical | + | +/- |
| Mucor | <37°C | Branched or unbranched, hyaline | – | +, in varying shapes | Spherical | – | – |
| Rhizomucor | 54°C | Branched, brown | – | Spherical | Spherical | + | – |
| Rhizopus | 45°C | Unbranched and brown mostly | Not prominent | Spherical or elongated | Spherical | + | – |
Laboratory Precautions
No special precautions other than general laboratory precautions are required.
Susceptibility
Few data are available on the in vitro susceptibility profile of Rhizopus spp. In an in vitro study comparing the in vitro activity of amphotericin B, ketoconazole, itraconazole, and voriconazole against strains of Rhizopus arrhizus, amphotericin B yielded low MICs [1130, 2432]. The MICs of ketoconazole, itraconazole, and voriconazole were comparable to eachother and slightly higher than those of amphotericin B [2432]. Voriconazole appeared to be less active than itraconazole in other investigators’ hands [1433]. Considerably high MICs were detected for fluconazole against Rhizopus arrhizus [689].
Among the novel antifungal agents, echinocandins such as
caspofungin and anidulafungin
appeared to have limited activity against this particular fungus [558, 1780]. On the other hand, azasordarin derivatives and posaconazole
were found to be active in vitro against Rhizopus arrhizus [1039, 1434]. Of note, posaconazole and ravuconazole appeared more active than voriconazole against Rhizopus [1782].
For MICs of various antifungal drugs for Rhizopus, see our N/A(L):susceptibility database.
Similar to the other genera belonging to the phylum Zygomycota, treatment of Rhizopus infections remains difficult. Due to its property to invade vascular tissues, infarction of the infected tissue is common and mortality rates are very high. Early diagnosis is crucial and surgical debridement or surgical resection, as well as antifungal therapy, are usually required. Amphotericin B is the most commonly used antifungal agent [408, 502, 696, 723, 1233]. Noteworthy, the addition of hyperbaric oxygen to amphotericin B did not have any improving effect on survival of experimental animals compared to amphotericin B alone or placebo air treatments [192]. Liposomal amphotericin B [696, 1004, 1470] and other lipid-based amphotericin B formulations such as amphotericin B colloidal dispersion [1588] have also been used in some cases with zygomycosis.
Clinical response to therapy is frequently unsatisfactory in zygomycosis [1656]. Reversal of immunosuppression is one of the most significant factors influencing the clinical outcome [1656]. Adjuvant therapy with cytokines, particularly the colony stimulating factors, has anecdotally been associated with better clinical response [805]. There are also a few data on successful use of fluconazole [1751] and terbinafine [1755] in treatment of zygomycosis, which require validation. Interestingly, fluconazole in combination with trovafloxacin or ciprofloxacin proved to be effective in a murine model of pulmonary zygomycosis [2185].