
Synonyms
San Joaquin Valley fever, Valley Fever, Desert Rheumatism

Arthroconidia
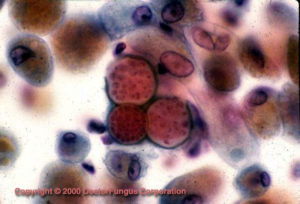
Spherules in tissue
Distribution in North America
Distribution in South America
Definition
Coccidioidomycosis is the infection caused by the dimorphic fungus Coccidioides immitis. The disease is endemic only in regions of the Western Hemisphere. In the United States, the endemic areas include southern Arizona, central California, Southern New Mexico, and west Texas. The endemic region extends southward into Central and South America. An arid climate, alkaline soils, hot summers, few freezings, and yearly rainfalls ranging between 5 to 20 inches characterize this area [1710]. Outbreaks occur following dust storms, earthquakes, and earth excavation where dispersion for arthroconidia is favored [86]. Coccidioidomycosis is acquired from inhalation of the spores (arthroconidia). Once in the lungs, the arthroconidia transform into spherical cells called “spherules”. An acute respiratory infection occurs 7 to 21 days after exposure and typically resolves rapidly. However, the infection may alternatively result in a chronic pulmonary condition or disseminate to the meninges, bones, joints, and subcutaneous and cutaneous tissues. About 25% of the patients with disseminated disease have meningitis [625, 626, 2158].
Forms of the disease
| CATEGORIES | NOTES |
|---|---|
| Asymptomatic |
|
| Acute Symptomatic |
|
| Chronic Pulmonary |
|
| Chronic skin disease |
|
| Joints / Bones |
|
| Meningeal Disease |
|
| Others |
|
Prognosis and therapy
Special resource: You may also want to refer to the Infectious Disease Society of America-Mycoses Study Group (IDSA-MSG) Practice Guidelines for this disease. It is available at the IDSA website.
Coccidiodomycosis includes a variety of illnesses many of which do not require therapy. Ninety-five percent of acute episodes resolve spontaneously. Nevertheless, follow up for 1 to 2 years is recommended for early identification of chronic pulmonary and extrapulmonary forms. Treatment should be given to patients with, or at high risk for, the more severe forms of the disease (see table) [795].
| Immunosupression |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adapted from [795]
Amphotericin B has often been used as initial therapy, but is increasingly being supplanted by therapy with an oral azole [795]. Ketoconazole, fluconazole and itraconazole have all been used. However, because of the toxicity profiles, the last two are preferred [796]. Length of therapy should be at least 1 year. Even after such a prolonged course of therapy, relapses are frequent [796]. Intrathecal amphotericin B has long been the standard therapy for meningeal disease [309, 1277], but fluconazole is increasingly found to be an effective and better tolerated option [795]. Surgical management could be of help in the treatment of pulmonary and extrapulmonary lesions [468, 793, 2008, 2134].
Histopathology
The tissue reaction is one of acute suppurative and granulomatous inflammation. Acute suppuration is usually present around the arthroconidia and after a spherule ruptures. Granulomatous inflammation usually occurs around developing spherules. Hyphae may be present in pulmonary cavities and meningeal lesions without arthroconidia, which can lead to confusion with the hyphae of an Aspergillus spp.
Laboratory
Direct examination
Direct examination of clinical specimens, such as fluids, sputa, and tissue in 10% KOH may show spherules 30-60 um in diameter with a thick wall (up to 2 um) and endospores 2-5 um in diameter characteristic of Coccidioides immitis. Endospores are released when the wall of the spherule ruptures. Endospores that are no longer in a spherule may remain close to each other, resulting in potential confusion with the yeast cells of Blastomyces dermatitidis. This is especially true if the spherule wall is no longer visible and the clinical specimen has been homogenized.
Isolation
Isolation involves inoculating the clinical material onto IMA agar, BHI agar with 10% sheep blood and a medium containing cycloheximide and incubating at 30°C. Cultures should be kept 4 weeks before discarding as negative. The fungus is fast growing and readily produces barrel-shaped arthroconidia 2.5-4 x 3-6 um with a disjunctor cell between each arthroconidium. Coccidioides immitis is a dangerous fungus and should be handled at all times with due respect in a Class II or III biological safety cabinet. It is classified as a BSL-3 agent. Laboratory confirmation of C. immitis is required because other fungi, such as members of the Gymnoascaceae, may develop an anamorph similar to Coccidioides. Useful in vitro identification procedures include special conversion media, exoantigen tests, and DNA probes. Slide cultures should not be set up when Coccidioides immitis is suspected due to its dangerous nature.
Natural habitat
Alkaline soil of the Lower Sonoran Life Zone in North, Central, and South America.
Susceptibility testing
Standardized testing procedures are not available. Microbiological resistance has not been demonstrated.