(described by Link in 1809)
Taxonomic Classification
Kingdom: Fungi
Phylum: Ascomycota
Class: Euascomycetes
Order: Eurotiales
Family: Trichomaceae
Genus: Penicillium

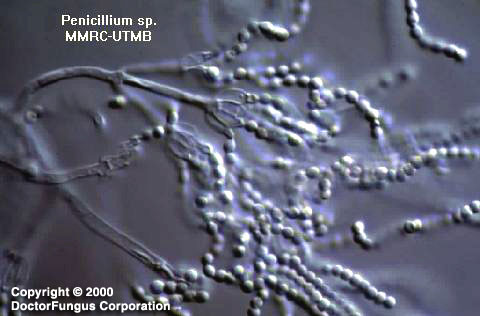
Penicillium spp.
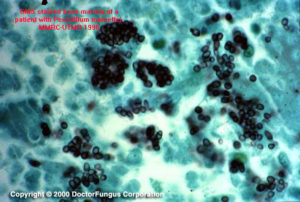
Penicillium marneffei yeast phase 35°C, GMS showing the intracellular yeast-like organism
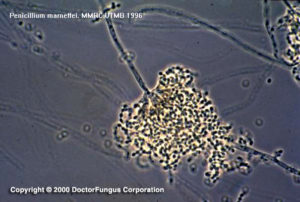
Penicillium marneffei at 25°C
Description and Natural Habitats
With only one exception (Penicillium marneffei, which is thermally dimorphic), the members of the genus Penicillium are filamentous fungi. Penicillium spp. are widespread and are found in soil, decaying vegetation, and the air. Showing again how it is distinct from other species in this genus, Penicillium marneffei is endemic specifically in Southeast Asia where it infects bamboo rats which serve as epidemiological markers and reservoirs for human infections.
Penicillium spp. other than Penicillium marneffei are commonly considered as contaminants but may cause infections, particularly in immunocompromised hosts. Penicillium marneffei is pathogenic particularly in patients with AIDS and its isolation from blood is considered as an HIV marker in endemic areas. In addition to their infectious potential, Penicillium spp. are known to produce mycotoxins [1805]. Some Penicillium spp. have telemorphs included in genera Eupenicillium, Talaromyces, Hamigera, and Trichocoma.
Species
The genus Penicillium has several species. The most common ones include Penicillium chrysogenum, Penicillium citrinum, Penicillium janthinellum, Penicillium marneffei, and Penicillium purpurogenum. Identification to species level is based on macroscopic morphology and microscopic features [531].
See the summary of species and synonyms for the Penicillium spp.
Pathogenicity and Clinical Significance
Penicillium spp. are occasional causes of infection in humans and the resulting disease is known generically as penicilliosis. Penicillium has been isolated from patients with keratitis [581], endophtalmitis, otomycosis, necrotizing esophagitis, pneumonia, endocarditis, peritonitis, and urinary tract infections. Most Penicillium infections are encountered in immunosuppressed hosts. Corneal infections are usually post-traumatic [581]. In addition to its infectious potential, Penicillium verrucosum produces a mycotoxin, ochratoxin A, which is nephrotoxic and carcinogenic. The production of the toxin usually occurs in cereal grains at cold climates [1804].
Penicillium marneffei is a pathogenic fungus and specifically infects patients with AIDS who live at or visit Southeast Asia (Thailand and adjacent countries, Taiwan, and India) where the fungus is endemic [565, 2114, 2200]. Penicillium marneffei infections have also been reported in non-AIDS patients with hematological malignancies and those receiving immunosuppressive therapy [2456]. Penicillium marneffei infection, so called penicilliosis marneffei, is acquired via inhalation and results in initial pulmonary infection, followed by fungemia and dissemination of the infection [431, 803, 1926, 2114]. The lymphatic system, liver, spleen and bones are usually involved. Acne-like skin papules on face, trunk, and extremities are observed during the course of the disease. Penicilliosis marneffei infection is often fatal.
Macroscopic Features
The colonies of Penicillium other than Penicillium marneffei are rapid growing, flat, filamentous, and velvety, woolly, or cottony in texture. The colonies are initially white and become blue green, gray green, olive gray, yellow or pinkish in time. The plate reverse is usually pale to yellowish [531, 1295, 2144, 2202].
Penicillium marneffei is thermally dimorphic and produces filamentous, flat, radially sulcate colonies at 25°C. These colonies are bluish-gray-green at center and white at the periphery. The red, rapidly diffusing, soluble pigment observed from the reverse is very typical. At 37°C, Penicillium marneffei colonies are cream to slightly pink in color and glabrous to convoluted in texture [531, 1295, 2144, 2202].
Microscopic Features
For species other than Penicillium marneffei, septate hyaline hyphae (1.5 to 5 µm in diameter), simple or branched conidiophores, metulae, phialides, and conidia are observed. Metulae are secondary branches that form on conidiophores. The metulae carry the flask-shaped phialides. The organization of the phialides at the tips of the conidiophores is very typical. They form brush-like clusters which are also referred to as “penicilli”. The conidia (2.5-5µm in diameter) are round, unicellular, and visualized as unbranching chains at the tips of the phialides [1295, 2144].
In its filamentous phase, Penicillium marneffei is microscopically similar to the other Penicillium species. In its yeast phase, on the other hand, Penicillium marneffei is visualized as globose to elongated sausage-shaped cells (3 to 5 µm) that multiply by fission.
Penicillium marneffei is easily induced to produce the arthroconidial yeast-like state by subculturing the organism to an enriched medium like BHI and incubating at 35°C, in which after a week, yeast-like structures dividing by fission and hyphae with arthroconidia are formed [531, 1295, 2144, 2202].
Histopathologic Features
Intracellular arthroconidial yeast-like cells are observed inside the macrophages in infected tissues [531].
Compare to
Paecilomyces
Gliocladium
Scopulariopsis
Penicillium differs from Paecilomyces by having flask-shaped phialides and globose to subglobose conidia; from Gliocladium by having chains of conidia; and from Scopulariopsis by forming phialides. Penicillium marneffei differs as well by its thermally dimorphic nature.
Laboratory Precautions
No special precautions other than general laboratory precautions are required.
Susceptibility
Available data are very limited. For Penicillium chrysogenum, MICs of amphotericin B, itraconazole, ketoconazole, and voriconazole are acceptably low, while the denoted MICs for Penicillium griseofulvum are higher than those for Penicillium chrysogenum [2432]. Notably, Penicillium marneffei isolates may yield considerably high MICs for amphotericin B, flucytosine, and fluconazole and relatively low MICs for itraconazole, ketoconazole, voriconazole, and terbinafine [531, 1094, 1152, 1489]. Further data are required to provide a more precise susceptibility profile for various Penicillium spp.
For MICs of various antifungal drugs for Penicillium, see our N/A(L):susceptibility database.
Amphotericin B, oral itraconazole, and oral fluconazole have so far been used in treatment of penicilliosis marneffei [431, 1371, 1926]. Oral itraconazole was found to be efficient when used prophylactically against penicilliosis marneffei in patients with HIV infection [423].